395 new diagnosis codes have been proposed by CMS for fiscal year 2024.
CMS recently released the fiscal year 2024 inpatient prospective payment system proposed rule, and with it came the annual proposed ICD-10-CM diagnosis code changes which include new codes to enhance the tracking and progression of Parkinson’s disease and more reimbursement for certain social determinates of health (SDOH).
The proposed rule includes 395 additions, 12 revisions, and 25 deletions to the ICD-10-CM diagnosis code set. If finalized, these changes will take effect October 1.
Of the 395 new ICD-10-CM codes, 123 of them are external cause codes to capture accidents and injuries. CMS also proposes 36 new codes for osteoporosis with current pathological pelvic fracture.
Other notable proposed code additions include:
Several new codes for sickle cell anemia
Five new codes for Parkinson’s disease with and without dyskinesia
Four new codes for migraine with aura
Three new codes for insulin resistance
When it comes to SDOH, the proposed changes would create two codes that indicate if a caregiver’s noncompliance is due to financial hardship or another reason. For example, the current code for “caregiver’s other noncompliance with patient's medication regimen” would become invalid and coders would use Z91.A41 (Caregiver's other noncompliance with patient’s medication regimen due to financial hardship) and Z91.A48 (Caregiver's other noncompliance with patient's medication regimen for other reason).
In the proposed rule, CMS also recognizes homelessness as an indicator of increased resource utilization. To compensate acute care hospitals for resources needed to care for patients experiencing homelessness, CMS proposes to increase the severity designation of three ICD-10-CM codes describing homelessness.
CMS invites the public to comment on all proposals. For more information on the rule, see the Federal Register. Comments are due to CMS no later than June 9.
Under the proposed rule, acute care hospitals that report quality data and are meaningful users of EHRs will see a net 2.8% increase in payments in FY 2024 (compared to 2023), an expected increase of $3.3 billion. However, disproportionate share hospitals could be facing a payment cut of $115 million.
Under this rule, hospitals may be subject to other payment adjustments under the IPPS, including:
Payment reductions for excess readmissions under the Hospital Readmissions Reduction Program
Payment reduction of 1% for the worst-performing quartile under the Hospital Acquired Condition Reduction Program
Upward and downward adjustments under the Hospital Value-Based Purchasing Program
CMS is also proposing health equity adjustments under the Hospital Value-Based Purchasing Program, which adjusts IPPS payments to acute care hospitals depending on their quality performance in the inpatient hospital setting. As part of its goal to measure policy impact more explicitly on health equity, CMS has proposed adding 15 new health equity hospital categorizations for payment impacts.
Hospitals may also see higher payments under a proposal to recognize homelessness as an indicator of increased resource utilization in the acute inpatient hospital setting. CMS proposed changing the severity designation of three ICD-10-CM diagnosis codes that describe homelessness from “non-complication or comorbidity” to “complication or comorbidity” to address the higher average resource costs of cases with these codes.
CMS has also proposed to allow rural emergency hospitals to be designated as graduate medical education training sites. This would enable more medical residents to train in rural settings amid worsening clinician shortages, especially in rural communities, CMS said.
Revenue cycle leaders should review the proposed rule and analyze the proposals’ potential impact on reimbursement and workflows. Changes could have a cross-functional impact, so it’s always important leaders ensure that all revenue cycle departments are aware of the proposed changes.
An enhanced EHR is key to a healthy revenue cycle, but one CMO says clinicians can't be left out of decision making and optimization.
HealthLeaderspreviously spoke with Michael Weiner, CMO of MSU Health Care, in East Lansing, Michigan, about a range of topics, including post COVID-19 clinical challenges and physician leadership, but there was one topic discussed that has been top of mind for revenue cycle leaders: optimizing the EHR.
HealthLeaders asked if there was anything specific that can be done to EHRs to make them more user friendly for clinicians, and according to Weiner, including clinicians in optimization and decision making is key.
“For example, when I see a patient, if I have to click 40 times to get from the beginning of the patient encounter to the end of the patient encounter, is there a more optimal way to do that? Is there a way to get through in 20 clicks? Is there a way for me to be able to dictate into the blocks I need to fill out to make it more efficient for me?” Weiner asked.
One solution Weiner said is offering advanced optimization training, which is having elbow-to-elbow experts working with the physicians as they see patients to improve their workflow within the EHR. Doing so will not only help the clinical team, but the patients too.
“There are also technologies that can make the experience better for clinicians and patients. We have adopted patient-supportive technology to make it easier to sign in, to make it easier to give medical history, and to avoid filling out pages of forms when you see a doctor. You can also bring in additional support such as scribes to help do the input work. We are looking at optimizing the electronic health record to improve retention and to make us a more attractive employer,” Weiner said.
When revenue cycle leaders look to update, implement, or optimize this software, the importance of including input from the clinical team was recently echoed by Liza Dzhezhora, healthcare IT analyst at Itransition.
“An EHR project’s success depends on more than just qualified developers; it also requires clinicians with industry-specific knowledge of hospital tasks, operations, and workflows. Hence, the EHR implementation project needs both technical and clinical perspectives,” Dzhezhora said.
According to Dzhezhora, revenue cycle leaders should select doctors with medium to high levels of computer competence (superusers), singling them out with the help of online tests. During the project, superusers should perform four essential tasks:
Workflow mapping. Superusers can map the selected workflows and regularly update them to make sure they fully reflect clinical processes.
Drafting the needed integrations. Through their awareness of existing digital solutions, superusers can map the necessary integrations and provide the information to the development team.
Usability testing. Superusers can identify issues that are potentially dangerous for patients, like wrong dosages or units of measurement.
Mentoring. Superusers can oversee beginners’ training, helping them master workflows and daily tasks.
“Doctors’ participation in the project can improve all clinicians’ understanding of the new EHR system and its place in their organization while making the implementation smoother,” Dzhezhora said.
The revenue cycle moves quickly, and so does its news.
Nearly 17% of in-network claims were denied by ACA marketplace plans in 2021.
Health insurers on the Affordable Care Act (ACA) marketplace denied an average of 16.6% of in-network claims in 2021, according to a brief by Kaiser Family Foundation.
Researchers analyzed data released by CMS on claims denials and appeals for qualified health plans (QHP) offered on HealthCare.gov for the 2021 plan year and found that denial rates ranged significantly from 2% to 49%. The dataset included 162 QHPs that reported receiving at least 1,000 in-network claims and showed data on claims received and denied.
Two out of three patients have never disputed a medical bill.
Patients don't usually contend medical bills, but when they do their chances of getting charges removed or reduced are high, according to a YouGov survey commissioned by revenue cycle firm AKASA.
Over 2,000 Americans were polled between March 9-14, 2022, including 179 adults with employer-sponsored high-deductible health plans, to gauge patient experience with disputed medical bills.
Nearly two-thirds of respondents (64%) reported having never challenged the validity or accuracy of a bill with their physician, hospital, or health insurance company. That figure shot up to 78% for uninsured individuals, while those with high-deductible health plans (45%) and Medicare Advantage (43%) were more likely to contend bills.
Healthcare execs eye workforce and back-office solutions in new AI study.
A new survey on the use of AI in healthcare finds that roughly half of the health systems surveyed are using the technology for back-office operations and workforce issues, and there's a lot of interest in conversational applications.
The survey of 40 leading healthcare executives, conducted by The Health Management Academy, sees growing support for AI "to fill gaps and improve productivity," according to a press release accompanying the report. And that growth is coming fast: Almost 85% of those now using AI for workforce issues expect a moderate to significant increase in one to three years.
Critical access hospitals, rural emergency hospitals, and other rural facilities should all take note of updated CMS guidelines.
As we know, it is essential for revenue cycle leaders to remain informed and compliant with the ever-changing CMS guidelines to ensure efficient reimbursement processes.
That being said, CMS recently released guidance on the proper billing practices, designations, and conversion processes for critical access hospitals (CAH) and rural emergency hospitals (REH). Remaining compliant with these designation and conversion processes will ensure your organization is getting the reimbursement it deserves.
Medicare-participating hospitals must meet several conditions to become and remain a CAH. CMS updated the location requirement for CAHs, specifying that they must be more than a 35-mile drive on primary roads from any other CAH or hospital.
A primary road is a numbered federal or state highway with two or more lanes each way, according to the guidance. CAHs in areas with only secondary roads available or mountainous terrain must be a 15-mile drive from other hospitals.
To establish a process for overseeing and resolving patient grievances, CAHs are now required to inform each patient of their rights before starting or ending care. In addition, CAHs must now have a unified and integrated quality assessment and performance improvement program if they are part of a multi-hospital health system.
The updated guidance also detailed the optional payment method for CAHs. “Under the optional payment method, the CAH bills facility and professional outpatient services only when physicians or practitioners have reassigned their billing rights to them,” said CMS. After physicians and practitioners reassign their billing rights to a CAH, they can’t bill for professional services.
CMS also included information on its newest provider type, REH. “REHs allow for emergency services, observation care, and additional medical and health outpatient services (if the REH elects to provide them) that don’t exceed an annual per-patient average of 24 hours,” said CMS.
REHs generally convert from a CAH or rural hospital with no more than 50 beds and don’t provide acute inpatient services, according to CMS.
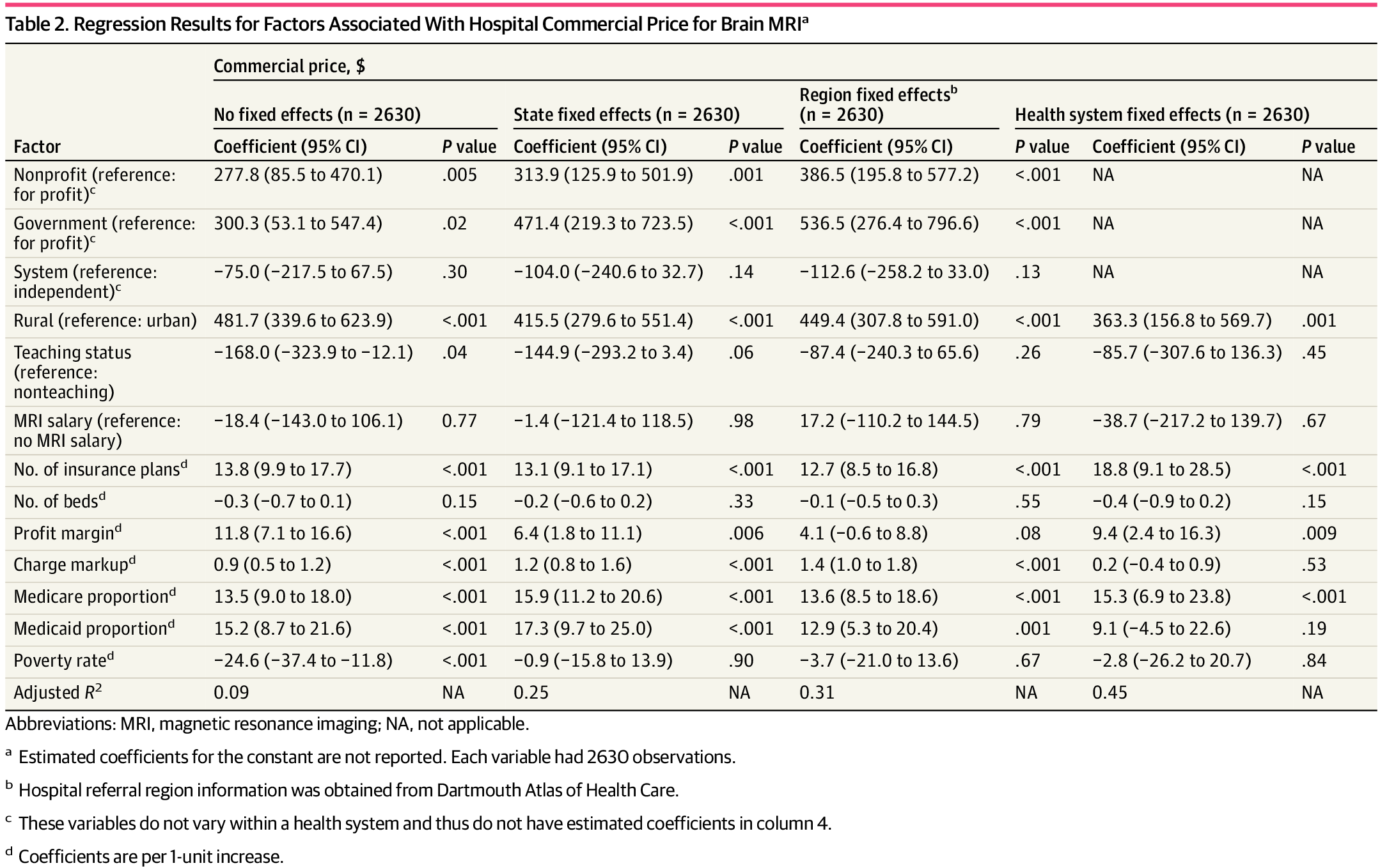
A new study shows nonprofit and government hospitals have higher commercially negotiated prices for MRIs than for-profit hospitals.
A study published in JAMA Open Network examined negotiated rates under the price transparency rule and has identified the most expensive type of hospital to receive a brain MRI among those that complied with the rule as of June 13, 2022.
The study leveraged new data associated with commercially negotiated prices nationwide to compare commercial rates for MRIs of the brain before and after contrast reported with CPT® code 70553. According to the study, nonprofit and government hospitals had higher commercially negotiated prices for brain MRIs than for-profit hospitals.
“Across the nation and within the same state, referral region, or health system, hospitals located in rural areas, contracting with more health plans, or treating more Medicare patients had higher prices, potentially reflecting these hospitals’ stronger bargaining power compared with insurers in their local markets,” the study said.
The sample contained 2,630 hospitals and found the following:
The median commercial price was $1,900 for nonprofit, system-affiliated hospitals in urban areas
Prices at nonprofit and government hospitals were $387 and $537 higher than the prices at for-profit hospitals
Photo courtesy of JAMA study ‘Factors Associated With Hospital Commercial Negotiated Price for Magnetic Resonance Imaging of Brain’
Since the hospital price transparency regulation went into effect on January 1, 2021, hospitals are required to make public their standard charges for items and services through a consumer-friendly display showing at least 300 shoppable services, as well in a machine-readable file.
Hospitals were slow to adapt out of the gates. In an assessment of 235 randomly sampled hospitals conducted by CMS between January and February 2021, 66% met consumer-friendly display criteria, 30% posted a machine-readable file, and 27% did both.
Those figures improved significantly in CMS' second assessment, this time of 600 randomly sampled hospitals between September and November 2022. The analysis found 493 hospitals (82%) posted a consumer-friendly display, 490 (82%) posted a machine-readable file, and 421 (70%) did both.
HealthLeaders' regulatory round up series highlights five essential governing updates that cover every aspect of the revenue cycle that leaders need to know. Check back in each month for more updates.
The revenue cycle is complex, detailed, and always changing, so staying on top of regulatory updates and latest best practices requires revenue cycle leaders' constant attention in this ever-changing industry.
In this revenue cycle regulatory roundup, there were an ample number of updates published by CMS and the OIG in March, including public health emergency (PHE) updates and OIG audits.
The OIG says the inability to identify denied claims in Medicare Advantage hinders its fraud oversight.
On March 2, the OIG published an issue brief regarding an evaluation into Medicare Advantage data and whether the lack of an indicator to identify payment denials in the data hinders efforts to combat fraud, waste, and abuse. CMS requires Medicare fee-for-service and Medicaid records for services to include denied claim indicators.
Medicare Advantage organizations (MAO) do not require indicators to identify a denied claim in MA encounter data, but MAOs are required to submit claim adjustment reason codes when MAOs do not pay the actual amount billed by the provider. The OIG reviewed 2019 MA encounter records to determine how many contained adjustment codes and whether they identified records that may contain payment denials. The OIG also interviewed and sent out questionnaires to involved parties about how they identify payment denials, how the lack of a denied claim indicator could impact audits and oversight work, and to determine why CMS does not require MAOs to submit this indicator.
The OIG found that the adjustment codes were used on almost all encounter records, but it was not possible to definitively determine which claims were denied using these adjustment codes. Oversight entities who spoke with the OIG said the denied claim indicator would make their efforts much easier and less burdensome. The CMS MA payment group said the indicator is not necessary and raised concerns about the potential burden on MAOs of requiring a denied claim indicator on encounter records.
The OIG noted, however, that the private companies which cover most MA enrollees are also involved in Medicaid managed care plans and therefore already have the ability to use denied claim indicators since they are required for Medicaid managed care plans. The OIG therefore recommends CMS require MAOs to definitively indicate on MA encounter data records when they have denied payment for a service on a claim.
There was an April 2023 update of the hospital outpatient prospective payment system (OPPS).
On March 10, CMS published a transmittal regarding the April updates to the OPPS. Updates include 23 proprietary laboratory analyses coding changes, a slew of updates to COVID-19 vaccine codes, updated language in the manual pertaining to various modifiers, and more.
The OIG released a COVID-19 PHE flexibilities end date.
On March 10, the OIG published a post regarding the end of its COVID-19 PHE flexibilities when the PHE ends on May 11.
The OIG outlined which flexibilities it put in place, what those flexibilities allowed, and when those will end. The flexibilities include refraining from subjecting providers to administrative sanctions for reducing or waiving cost-sharing obligations for telehealth services, exercising certain enforcement discretions in order not to impose administrative sanctions for certain remuneration related to COVID-19 that was covered under blanket waivers, and more.
Medicare improperly paid physicians for spinal facet-joint interventions, the OIG says.
The OIG published a review of whether Medicare paid physicians for spinal facet-joint interventions in accordance with Medicare requirements.
The OIG had previously found that Medicare improperly paid for these services, and it noted that facet-joint interventions are at risk for overutilization. This audit was conducted as a follow-up to previous audits, and it examined interventions from August 1 through October 31, 2021.
The OIG found that Medicare did not pay physicians for selected facet-joint intervention sessions in accordance with Medicare requirements, as 66 of the 120 sampled sessions did not comply with at least one–if not more–of the requirements.
Of the 120 sampled sessions, the OIG also found that 43 had claim lines that were billed for at least one therapeutic facet-joint injection, and 33 of those sessions should have been billed for diagnostic instead of therapeutic injections. This did not result in improper payments because the payments for therapeutic injections are the same as the payment for diagnostic injections. However, the 66 sampled facet-joint intervention sessions deemed to be paid in error totaled $18,084 in improper payments.
The OIG recommends CMS direct the MACs to recover the $18,084 in improper payments. The OIG also recommends CMS develop collaborative training programs to be used for all MAC jurisdictions and develop solutions to prevent the incorrect billing of diagnostic facet-joint injections as therapeutic facet-joint injections. CMS concurred with the OIG’s recommendations.
There was a Medicare Advantage compliance audit of Geisinger Health Plan, and it could cost Geisinger half a million dollars.
On March 20, the OIG published a review of whether select diagnosis codes that Geisinger Health Plan submitted to CMS for use in the risk adjustment program complied with federal requirements.
The OIG conducted the audit by sampling 270 unique enrollee-years across nine groups of high-risk diagnosis codes for which Geisinger received higher payments for 2016 and 2017. The OIG found that diagnosis codes for 224 of the 270 enrollee-years did not comply with federal requirements because there was not sufficient support for those codes in the medical records or Geisinger could not find the medical records to support the diagnosis codes. The OIG found that based on the results of the sample, Geisinger received at least $566,476 in net overpayments in 2016 and 2017.
The OIG recommended that Geisinger refund the federal government for the $566,476 in overpayments, identify and return similar overpayments, and examine its existing compliance procedures to identify areas where improvements can be made to ensure diagnosis codes at high risk for being miscoded comply with federal requirements. Geisinger disagreed with all of the findings and recommendations in the report, but the OIG stood by its findings.
The new diagnosis codes, which became billable on April 1, place a heavy focus on social determinants of health (SDOH).
For example, there is now a new SDOH code for reporting problems related to education and literacy is among the code additions.
Also added are codes to update the verbiage related to critical perpetrator of abuse external cause codes with that of current CDC core data collection elements and literature related to patient maltreatment and neglect — including elder abuse.
There is also a slate of new codes pertaining to “financial abuse” of adults and children. For example, the April update brings a code for adult financial abuse, confirmed, initial encounter and a code for child financial abuse, confirmed, initial encounter.
The ICD-10-CM Official Guidelines for Coding and Reporting have also been expanded to provide more examples in the SDOH section. These updates aren’t surprising since, with increasing attention on population health and quality initiatives, organizations have turned their focus on SDOH and how capturing those ICD-10-CM codes impacts their patient population and their success in caring for that population.
Aside from the new ICD-10-CM codes from the CDC, CMS also implemented 34 new ICD-10-PCS procedure codes as part of a quarterly update to the code set (which also became effective April 1).
Because coding occurs mid-cycle, it provides an opportunity to catch errors introduced earlier in the process, as well as preventing similar errors in the future.
Staying abreast of these regulatory coding updates is important for revenue cycle leaders as coding—and its completeness and accuracy—has a profound impact on an organization's bottom line.
Not many regulations have had such a profound impact on patients and organizations like prior authorization requirements.
Prior authorizations involve complex, time-consuming processes which put a huge administrative burden on revenue cycle staff. Not only that, but the requirements for prior authorizations can vary between insurance plans, leading to confusion and additional administrative tasks which can take time away from patient care.
Staying up to date on regulatory changes is key to helping to reduce these burdens for your staff. Here are five recent stories on prior authorizations that revenue cycle leaders can’t miss.
Prior auths 'delay, deny, and disrupt': Major medical societies show support for reform
118 major organizations, spanning from the American Medical Association to The Alaska State Medical Association, sent a letter to CMS urging it to finalize proposed prior authorization reforms that target the inappropriate use of authorization requirements by Medicare Advantage plans which, the organizations say, delay, deny, and disrupt the provision of medically necessary care to patients. Read the story here.
Physicians say prior authorization hurts patient outcomes, wastes resources
The recent poll of 1,001 practicing physicians in December 2022 reveals the ramifications patients and providers have to deal with from health insurers imposing prior authorization practices to control costs.
Nearly nine in 10 respondents (89%) said that the administrative process had a negative impact on patient clinical outcomes, with only 2% answering that it has any positive impact. Read more here.
Hey senate, want to help rev cycle workforce shortages? Reduce prior auth requirements, support tech
The Senate Health, Education, Labor, and Pensions Committee recently published a request for information on the drivers of healthcare workforce shortages and potential solutions. The request garnered responses from several large medical associations with solutions aimed at prior authorization requirement reduction and more support in automation.
When it comes to prior authorizations, the MGMA said in its feedback that in order to address the multi-faceted causes of physician and staff burnout, Congress should examine legislative solutions to ease administrative burden and allow providers to focus on patient care, including prior authorization reform. Read the full story here.
Feds move to rein in prior authorization, a system that harms, frustrates patients
Originally focused on the costliest types of care, such as cancer treatment, insurers now commonly require prior authorization for many mundane medical encounters, including basic imaging and prescription refills. In a 2021 survey conducted by the American Medical Association, 40% of physicians said they have staffers who work exclusively on prior authorization.
So today, instead of providing a guardrail against useless, expensive treatment, pre-authorization prevents patients from getting the vital care they need, researchers and doctors say. Read more here.
Ophthalmologists ask CMS to suspend certain prior auth policies
In recent comments to CMS, the American Academy of Ophthalmology addressed CMS’ proposed rule regarding improving the electronic exchange of healthcare data, particularly in terms of addressing Medicare Advantage prior authorization processes, an area of the rule that the group says has a profound effect on patients. Read the full story here.
Revenue cycle leaders must review, update, and optimize their EHR systems regularly to ensure their efficiency over time.
Revenue cycle leaders are on the hook for ensuring their organization can maximize reimbursement, minimize revenue leakage, and improve patient care, and one sure-fire way to make sure this happens is through an optimized electronic health record (EHR) system.
As we know, having an optimized EHR system reduces the risks of lost or incomplete documentation, billing errors, and slower reimbursement. Additionally, improving the quality and accuracy of patient medical data can enhance the quality of care and reduce medical errors.
Whether heading up an EHR implementation for the first time, in the process of switching vendors, or working to update and review your current system, by streamlining implementation, revenue cycle leaders can ensure a smoother transition to an updated system and achieve a variety of benefits for both the organization and patients.
While easy in theory, EHR deployment is not a one-time effort but a continuous process that needs to reflect changes in industry trends and care provision methods.
As Liza Dzhezhora, healthcare IT analyst at Itransition, said in our sister publication PSQH, revenue cycle leaders must review, update, and optimize their systems to ensure their efficiency over time.
Dzhezhora shared a step-by-step plan with readers that covered critical aspects of a future proof EHR implementation. Here is what she had to say:
Step 1: Project planning and preparation
To properly plan out a future EHR, revenue cycle leaders needs to take these preparatory actions:
Assess the current EHR system, collecting clinicians’ feedback and identifying their core pain points.
Evaluate users’ needs and requirements and arrange them by priority. This can help to avoid a common EHR project pitfall: wasting a lot of time on developing a function that is not currently relevant.
Ensure strong leadership from the stakeholders representing each group interested in EHR implementation, like board members, clinicians, marketers, and administrative personnel. Additionally, you should start promoting the new system’s benefits early on to mitigate staff resistance, a factor that accompanies change.
Step 2: A multidisciplinary team setup
An EHR project’s success depends on more than just qualified developers; it also requires clinicians with industry-specific knowledge of hospital tasks, operations, and workflows. Hence, the EHR implementation project needs both technical and clinical perspectives.
Revenue cycle leaders should select doctors with medium to high levels of computer competence (superusers), singling them out with the help of online tests. During the project, superusers should perform four essential tasks:
Workflow mapping. Superusers can map the selected workflows and regularly update them to make sure they fully reflect clinical processes.
Drafting the needed integrations. Through their awareness of existing digital solutions, superusers can map the necessary integrations and provide the information to the development team.
Usability testing. Superusers can identify issues that are potentially dangerous for patients, like wrong dosages or units of measurement.
Mentoring. Superusers can oversee beginners’ training, helping them master workflows and daily tasks.
Doctors’ participation in the project can improve all clinicians’ understanding of the new EHR system and its place in their practice while making the implementation smoother.
Step 3: EHR system implementation
EHR implementation is a multistep process that includes several iterations of testing and debugging, followed by rollout. But before the rollout occurs, the IT team needs to choose a suitable approach: a big-bang deployment or a phased deployment.
A big-bang deployment involves immediate go-live across the healthcare facility. This tactic is fast and efficient, allowing clinicians to begin using the new system at once. However, it is only optimal for superusers and could overwhelm clinicians with below-average computer skills. A phased deployment rolls out EHR system features incrementally. For example, providers can launch their EHR in one department and then gradually deploy it across the facility. This allows users to get acquainted with the EHR at their own pace.
Step 4: Plans for the future
EHR implementation doesn’t end with go-live. The team will also need to perform regular system optimization. This usually involves three steps:
Updating the EHR feature set and workflows
Adding new integrations
Removing underused features
Leaders should plan to start on first optimizations three months after EHR rollout.
EHR implementation challenges to expect
Unfortunately, even a well-planned EHR implementation can be riddled with issues, including initial workflow disruptions and burnout among clinicians.
Fortunately, these issues are manageable. To overcome them swiftly, leaders need to:
Set up a support sub-team comprising superusers and tech experts from the IT vendor’s side to be available for support 24/7. This can lower doctors’ stress levels, as they will know they can get help at all times. For example, Valley Children’s in California deployed a new EHR during the pandemic. To prevent coronavirus exposure for the team, they set up a virtual help line for EHR implementation, where pediatricians could call and get help with EHR-related issues.
Initially, assign patients to clinicians with regard to their computer skill levels (i.e., give lesser workloads to clinicians with lower skill levels) to reduce clinicians’ stress and minimize burnout risk.
Inform clinicians about the ongoing hurdles and their resolution during the first month.
Ensure a user-friendly training model. A complicated or confusing EHR training program will increase physicians’ stress, so it makes sense to have a program that is intuitive and engaging, and to interview clinicians and nurses on their training preferences. For instance, Southern Ohio Medical Center in Portsmouth set up at-home training through their vendor to help staff train efficiently while following social distancing requirements. Thanks to the vendor’s efforts, the Center was able to provide in-person support and monitor the progress of their clinicians’ home training.