The American Medical Group Association (AMGA) raised concerns about the good faith estimate (GFE) process and how it is creating an administrative burden for medical groups.
In a letter to CMS, AMGA members said GFE requirements have resulted in significant challenges for providers to effectively schedule, coordinate, and deliver care.
AMGA members report completing more than 45,000 GFEs in a month and expect that number will increase, according to the association.
"The current GFE requirements impose additional stress to an already strained healthcare workforce," said AMGA president and CEO Jerry Penso. "CMS should reform the process so that the estimates provide the information patients need without creating new administrative obstacles for providers to overcome."
The AMGA says it applauds HHS' efforts to promote transparency but believes there is a misunderstanding as to the infrastructure needed to satisfy GFE requirements in a timely matter.
In the letter, AMGA members say their concerns stem from three key areas:
Unclear guidance: Guidelines issued to providers are either confusing or conflicting, and providers have raised questions about the circumstances necessitating the delivery of a GFE to a patient
Staffing constraints: AMGA members report that non-medical staff are required to allocate a significant number of hours to complete GFEs
Cost and infrastructure barriers: AMGA members report a significant expense associated with completing GFEs
In line with the cost and infrastructure barriers, the AGMA says there is currently no realistic way to complete GFEs electronically.
"Members are developing workflows and infrastructure to support GFEs, but doing so diverts scarce resources from other priorities, particularly during the ongoing public health emergency. This includes reassigning staff from other duties to complete GFEs," the letter says.
The AMGA recommends that CMS work with stakeholders to develop a process in which GFEs are beneficial for patients, while not causing additional administrative burdens to providers.
HealthLeaders' new series highlights five essential governing updates that cover every aspect of the revenue cycle that leaders need to know. Check back in each month for more regulatory updates.
The revenue cycle is complex, detailed, and always changing, so staying on top of regulatory updates and latest best practices requires revenue cycle leaders' constant attention in this ever-changing industry. In this revenue cycle regulatory roundup, there were an ample number of updates published by CMS and the OIG in May, including studies on prior authorization requests and patient harm.
Here are the five updates you need to know.
1. Even the OIG has prior authorizations on the mind.
The OIG published a reportregarding whether Medicare Advantage Organizations (MAO) are appropriately approving or denying services which require prior authorizations: What it found was not great and has even set off the American Hospital Association (AHA).
The OIG looked at a stratified random sample of 250 denials of prior authorization requests and 250 payment denials issued by 15 of the largest MAOs in June 2019.
It found that 13% of the prior authorization requests that the MAOs denied actually met Medicare coverage rules. The two common causes of those denials were MAOs using clinical criteria for medical necessity beyond what Medicare has in its coverage rules and MAOs stating that prior authorization requests did not have sufficient documentation to support approval when the OIG’s reviewers said the documentation provided was more than sufficient to support the request.
The OIG also found that 18% of the payment request denials met Medicare coverage rules and MAO billing rules. The OIG attributed most of these denials to human error and system processing error.
The OIG recommends CMS issue new guidance on the appropriate use of MAO clinical criteria in medical necessity reviews, update its audit protocols to address issues identified in this report, and direct MAOs to take steps to identify and address vulnerabilities that can lead to manual review errors and system errors. CMS agreed with all recommendations.
Because of this, the AHA is calling on the Department of Justice (DOJ) to establish a task force to conduct investigations into health insurance companies that routinely deny patients access to care and payments to providers.
In a letter to acting assistant attorney general Brian Boynton, the AHA states that it is time for the DOJ to exercise its False Claims Act authority to penalize MAOs that restrict services to beneficiaries, citing this OIG report.
2. Patient safety for the Medicare population is in the spotlight.
The OIG published a report regarding adverse events in hospitals in October 2018. The report is a repeat of one that was published in 2010 that looked at patient harm in October 2008.
In this newer report, the OIG found that 25% of Medicare patients experienced patient harm during their hospital stays in October 2018.
Physician reviewers determined that 43% of these harm events could have been prevented if patients had been provided better care. Of the 25% of patients who experienced harm, 12% of patients experienced adverse events that led to longer hospital stays, permanent harm, life-saving intervention, or death. The other 13% of patients experienced types of harm that were temporary and required intervention but did not have longer-lasting effects. The most common types of harm events were related to medication (43%) and patient-care issues (23%).
The OIG noted that while HHS has taken steps in the past to improve patient safety in hospitals, it must do more. The OIG issued seven recommendations, three of which applied to CMS.
Those included recommendations that CMS update and broaden its lists of hospital-acquired conditions to capture common, preventable, and high-cost harm events; explore expanding the use of patient safety metrics in pilots and demonstrations for health care payment and service delivery; and develop and release interpretive guidance to surveyors for assessing hospital compliance with requirements to track and monitor patient harm.
3. Be on the lookout for potential hospital outpatient payment changes.
CMS published a transmittalregarding the July 2022 updates to the hospital outpatient prospective payment system. Updates include a new code for the over-the-counter COVID-19 test demonstration, four new procedures assigned to new technology ambulatory payment classifications, and more.
It’s important for revenue cycle leaders to keep an eye on the OPPS as it’s also tied to price transparency regulations. For example, in the 2022 OPPS final rule, CMS increased price transparency penalties.
4. The Joint Commission will continue to be the CMS’ hospital accreditation program of choice.
CMS published a final noticein the Federal Register to announce its decision to approve The Joint Commission for continued recognition as a national accrediting organization for hospitals that wish to participate in Medicare or Medicaid.
5. You may be off the hook from a full-scale emergency exercise.
CMS revised a memorandum to state survey agency directors regarding clarifications on testing exercise requirements in light of the COVID-19 public health emergency (PHE).
Due to the continued PHE and the number of facilities still operating under disaster/emergency conditions, CMS is exempting any inpatient or outpatient facility still operating under an activated emergency from the full-scale exercise requirement for specified 12-month cycles of testing exercises. Revisions add information for outpatient providers and revised the information on individual facility-based exercises and important reminders.
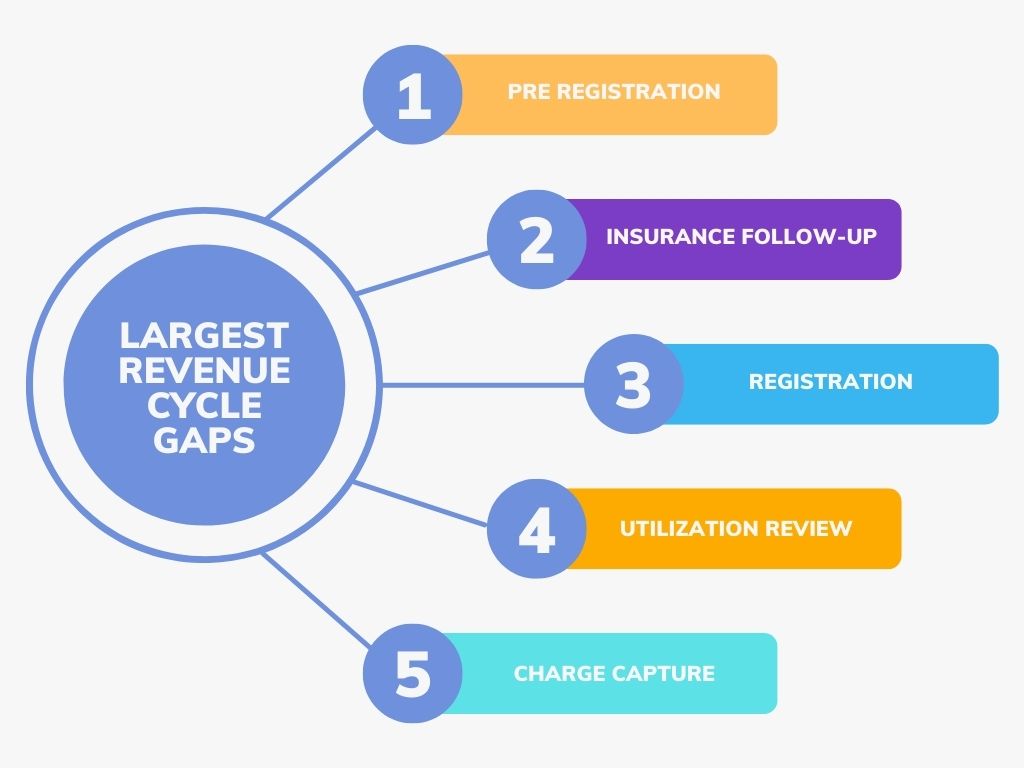
At the HealthLeaders Revenue Cycle Exchange, which was recently held in Louisville, Kentucky, revenue cycle leaders opened up about gaps they are seeing in their department.
Pre-registration difficulties were top of mind at the recent HealthLeaders Revenue Cycle Exchange. When asked to identify areas that see the biggest gaps in their revenue cycles, 68% of the leaders pointed the finger at pre-registration. Another area of difficulty is insurance follow-up, as 64% of attendees marked this as a gap in their operation.
Other concerns among this group of prominent VPs and directors include registration and utilization review, as 56% and 52% of leaders, respectively, flagged these areas as pain points within their organizations.
These trends aren’t surprising, as most of these sectors within the revenue cycle have been linked to staffing shortages and automation challenges.
For example, echoing the same gaps as leaders at the Revenue Cycle Exchange, a recent survey, which included responses from 400 healthcare financial leaders, ranked registrars, billing specialists, and patient follow-up staff as the most in-demand positions within the revenue cycle.
The American Hospital Association also recently declared its frustration with pre-registration and other front-end revenue cycle processes, not only due to staff shortages but also the lack of automation.
It’s no surprise that when asked what top trends they are focused on in the immediate future, most (83%) executives at the event cited automation and/or technology.
Other immediate areas of focus were data/analytics and improved financial performance with 58% and 66% of attendees choosing these areas, respectively.
The HealthLeaders Exchange is an executive community for sharing ideas, solutions, and insights. Please join the community at our LinkedIn page.
To inquire about attending a HealthLeaders Exchange event, email us at exchange@healthleadersmedia.com.
The Office of Inspector General recently audited the Department of Veterans Affairs' (VA) EHR implementation and found problems with its current data migration, interface usage, and user access.
After a series of problems and delays in the VA's implementation of a new EHR modernization (EHRM) program, more issues have surfaced despite the departments’ efforts.
The EHRM program was created to connect and improve data exchange between the Department of Defense (DOD), the VA, and external health providers.
According to the audit, the goal of its implementation is to increase EHR interoperability and create the ability to exchange EHRs securely with other HIT systems without special effort on the part of the user.
The audit states that the DOD and VA did not take all needed actions for interoperability, however, possibly in part because the oversight committee (FERHM) had little active engagement in the program.
According to the audit, the office failed to:
Consistently migrate patient information to create a single, complete patient EHR
Develop interfaces from all medical devices so patient information will automatically upload to the system from those devices
Ensure that users were granted access to the software for only the information needed to perform their duties
The audit recommended the FERHM program director develop and implement plans to create interfaces for medical devices that will easily connect and transfer data to the new EHR platform, modify user roles to better limit patient information, migrate patient information after defining the type of healthcare information that constitutes a complete EHR, and more.
The patient financial experience is just as important to a hospital as a patient's clinical experience. Healthcare leaders share their thoughts on current billing challenges and solutions.
Editor's note:This article appears in the March 2023 edition of HealthLeaders magazine.
Revenue cycle leaders must pay attention to each aspect of an organization's revenue cycle to have a prospering organization. Although there is an individual argument for streamlining each segment of the cycle, when it comes to improving the patient financial experience, it's imperative to put the microscope on an organization's current billing process.
Chris Johnson, vice president of revenue cycle at Atrium Health, and Chris Cox, senior vice president of product, strategy, and operations at iVitaFi, recently spoke at the HealthLeaders Patient Financial Experience NOW Summit about challenges they are seeing in the industry when it comes to the billing process and proactive ways to solve these challenges.
"We often hear in the industry that the patient experience was great and everything was phenomenal, then the patient gets the bill and all of the sudden the perception of the services received can change which impacts the patient financial experience," Johnson said.
As Johnson said, this shows that improving the billing experience can drive up satisfaction scores and an overall positive patient experience for an organization. Cox added that the patient billing experience affects how the patient ultimately feels about their experience at that organization, regardless of how the clinical care went—so it's important to remedy when it comes to patient leakage.
"Providers lose, on average, between 10%–30% of revenue as a result of patient leakage, and that's hundreds of millions of dollars in losses per year," said Cox.
Examining the challenges
So where should organizations start when looking to improve this patient experience?
"There are quite a few challenges in the market today when it comes to a patient's billing experience," said Johnson. Narrowing down those challenges and working on perfecting them will ensure a positive patient financial experience.
When it comes to a patient's bill, it's common for certain populations to find the amount of information presented overwhelming.
"Healthcare billing continues to be a complex process especially since you have the provider, patient, and payer all involved," said Johnson. "Quite frankly, when some patients see an insurer's use of CPT and ICD-10-CM codes, it can be like a foreign language, and it can cause real confusion."
Another added component seen across the healthcare industry is that patient bills still tend to show gross charges for the service or services provided to a patient.
"While gross charges are not the actual amount paid by insurers or patients, we continue to use them for billing purposes across our industry. Providers often assume patients are not concerned about gross charges, but this may not be the case." Johnson said.
"When we send a patient an itemized bill and they see their gross charges for $100,000—all of the sudden they are interested in those gross charges, not just what their actual financial responsibility is. So again, I think billing continues to be more complex than it needs to be as an industry," he said.
Price transparency has come a long way in the industry, but certain populations may need more education on what they are seeing in that final bill and breaking down this overload of information is an important step in achieving a positive patient financial experience.
"I see it time and time again where throughout the continuum of care, the billing aspect of service is just not discussed. And even when a patient would proactively ask, 'How much does this cost?' that discussion goes 'Oh no, we'll just send you a bill,' " said Cox.
Bringing that conversation forward and setting the expectation that a patient may see a gross charge or mentioning to a patient that they haven't met a deductible will help remove that surprise element from the patient's bill, Cox said.
On top of this surplus of coding and pricing information, it's not unusual for patients to receive multiple bills from different providers for one episode of care.
"That can be confusing for patients. And again, it's not a problem that we have successfully fixed at this point," said Johnson.
Also, it's common for a patient's statement to not completely align with the explanation of benefits that the patient receives from their insurance company. Receiving multiple bills for one encounter as well as receiving mismatched facility and payer statements can greatly affect the patient's financial experience.
"While we are continuing to improve and provide better information to our patients, we have a more ground to cover in making this industry and process truly patient-friendly," Johnson said.
Potential solutions
So, what can organizations focus on to improve the patient financial experience?
Being able to articulate to patients how much they owe in a clear and concise manner is critical and has been brought to the forefront by the No Surprises Act. An opportunity to improve a disconnect in communication can start as early as patient scheduling, check in, or check out.
"Providing this information to patients at all of those different touch points, having that discussion with the patient, and just setting the right expectations can improve that patient financial experience," Cox said.
Another solution to improve on the billing and collection process is simply having those back-end staff be more friendly and understanding, said Cox.
"I've never received a phone call where I pick up the phone and I'm like, 'Hey, you caught me at a great time. I'm so happy you called me,'" said Cox.
"All times are equally inconvenient for patients, and finding a better medium to contact patients or even giving them the ability to schedule a call through text and say, 'Would you like to schedule a call with us to discuss your bill?' Those are some areas where I think we could make it a little bit more friendly and ultimately improve the financial results of this process," he said.
Johnson agreed and added that although burdensome to some hospitals, the move toward price transparency is only going to help improve that patient financial experience, especially when patients are educated on the information they are being presented.
"I know it's been a difficult journey for a lot of us, and the rules that require us to do some of this don't always line up with reality of either what we can do or what needs to be done. But I still believe that it should be considered a positive thing because, ultimately, it's going to give patients more information about what they will ultimately owe out of pocket and options for resolving the out-of-pocket expense," Johnson said.
The revenue cycle space is seeing a boom in automation and technology, giving patients better access to patient portals, digital front doors, and payment options.
While patients may be getting an information overload through their bills and statements, once this information is paired down and streamlined, the advancement of technology can make the patient financial experience easier and more transparent.
Johnson echoed this point by saying that "healthcare has been providing more and more information to the patients through online portals. We are moving down multiple payment paths, trying to make that a component of the patient experience as easy as it can be."
"The ultimate goal is to give the patient the information they want, when they want it, where they want it, and how they want it, including the ability to make payments and to interact with us on their financial issues in any manner that they see fit," he said.
The growth of more payment plan options have also been a key solution in bettering the patient financial experience. Most organizations are dealing with patients who have higher out-of-pocket expenses, and it's becoming more likely that patients are routinely unprepared to pay the out-of-pocket expenses.
"When you carry $3,000, $5,000, or $10,000 out-of-pocket maxes, most patients aren't walking around with either that kind of money or the ability to write a check at one point in time. And I think the industry is responding to that, and providers are responding to that to try to make the payment mechanism for those out-of-pocket expenses easier for patients to navigate," Johnson said.
Finding solutions to these common patient billing pitfalls is imperative for organizations.
"The mindset should be that the patient financial experience needs to follow the same path as the clinical experience," Johnson said. "They both need to be phenomenal in order for our patients to be satisfied with the organization providing the service."
"It's important that we're setting the right expectations so that way when patients get a bill, they're not surprised. We want patients to not only pay their bill, but we want them to come back. That patient leakage is incredibly important to track and monitor, and organizations need to have a plan on how to minimize it moving forward," Cox said.
Revenue cycle leaders at the Revenue Cycle Exchange in Louisville, Kentucky, shared solutions to improving the remote work experience for their staff.
Managing a remote workforce was top of mind at the HealthLeaders Revenue Cycle Exchange, which is underway this week in Louisville, Kentucky.
Remote work poses challenges, and revenue cycle leaders shared some of the solutions they've implemented at their own organizations to improve the remote work experience for everyone involved.
Here are some of the challenges and solutions to managing a remote or hybrid workforce that leaders were busy examining.
The challenge: Deciding on a permanent work model
Since the beginning of the pandemic, remote work has become the norm and revenue leaders are finding themselves at a crossroads in deciding between permanently offering a fully-remote, in-office, or hybrid workforce model.
While some leaders are still holding on to an in-office model, most revenue cycle leaders at the Exchange are seeing an outcry for a permanently remote model from their staff.
And while leaders are seeing that the younger generation are pushing for a permanently remote position, older staff are happy with working in-house.
The solution: Offer something for everyone
Leaders at the Exchange made it clear that it’s important to offer a little something for everyone, this means offering both remote and in-office work to those who meet set expectations.
One revenue cycle leader shared that their organization recently started implementing “hoteling” for those who would like to work in-house as they maintain an almost entirely remote staff.
When it comes to remote work, hoteling involves signing up or booking access to a workspace, much like at an actual hotel. Even in a room full of empty desks and unoccupied workstations, a person has to check in with central booking to access their spot, which makes this model more structured than a first-come, first-served model.
Offering models like this allows those who want to come into an office access to do so, while allowing those who prefer remote work to stay at home.
Leaders are also seeing shifts on preferences based on generational differences. Younger staff are more likely to want to come into an office while older staff are happier at home, leaders said.
Offering something for everyone who meets productivity measures is a great way to ensure positive moral.
The challenge: Engaging staff
Although virtual huddles and meetings are a great way to keep staff engaged, they only work if everyone in the meeting is fully participating.
Leaders also said that they have tried hosting on-site activities, but with little engagement from staff.
The solution: Tailoring engagement strategies per demographic
Being physically apart means doubling down on communications, including formalizing huddles and having regular leadership-level check-ins, and while older employees may find this engaging enough, leaders are seeing that newer, younger employees are struggling without face-to-face interactions when trying to navigate their new career.
One leader mentioned that their organization created a more robust social media experience in order to create a community for that younger staff.
Tailoring engagement strategies has been key for a lot of organizations when it comes to creating a positive work environment that bridges generational gaps.
Stay tuned in the coming days and weeks for more key takeaways from the Revenue Cycle Exchange.
The HealthLeaders Exchange is an executive community for sharing ideas, solutions, and insights. Please join the community at our LinkedIn page.
A focus on front-end revenue cycle efficiency can help to avoid costly medical necessity denials.
Denials are at the top of mind for revenue cycle leaders, and it’s not uncommon for denials to come from one source within your front-end revenue cycle: medical necessity decision-making.
Four words often describe the efforts to prevent denials related to medical necessity: too little, too late. Mistakes are made early in the patient's hospital stay, and these mistakes lead to problems down the road.
Tiffany Ferguson, LMSW, ACM, and Marie Stinebuck, MBA, MSN, ACM, CEO and COO at Phoenix Medical Management, Inc., discussed why the best strategy to prevent these denials is a proactive approach that focuses on front-end revenue cycle processes at a recent NAHRI virtual event.
"If we get it right and we really focus on that front-end revenue cycle process for efficiency, we probably don't need to have so many work queues and corrections on that back end," Ferguson said.
A recent Change Healthcare report comparing 2020 data to 2016 data found a 23% increase in Medicare claim denials, half of which were related to front-end revenue cycle issues. And about 86% of those denials were preventable.
"The top areas that they identified as having issues were registration and eligibility data that was missing or invalid claim data," said Ferguson. These issues included authorization for pre-certifications, services not covered, and medical necessity. This reinforces the need to get things right during registration, scheduling, benefit verification, and front-end collections, she said.
"Medical necessity is required to determine whether the care provided to a patient is medically necessary, must be done in a hospital setting, and is reimbursable by the payer source," said Stinebuck.
While payer definitions of medical necessity can vary, what doesn’t change is the need to clearly spell out in the medical record why a patient needs hospital-level care.
"Documentation of medical necessity justifies the necessity of acute care through complex medical decision-making," said Stinebuck.
Physician documentation must show the acuity of the patient's condition and any comorbidities that relate to why this patient needs to be in the hospital. It should clearly show why the patient needs hospital-level care and why that care can’t be performed elsewhere.
Revenue cycle leaders should work closely with their revenue cycle directors and managers to shore-up these types of inefficiencies within their workflow. Avoiding medical necessity denials through these missteps will directly contribute to the overall health of an organization.
After appealing the courts' ruling on vacating a piece of arbitration within the No Surprises Act, HHS asks the court for a hold on its plea.
HHS recently requested for a hold on its appeal of a Texas federal court ruling vacating parts of the independent dispute resolution (IDR) process in the surprise billing interim final rule.
According to the American College of Emergency Physicians (ACEP), HHS filed an appeal, but later asked the court to hold its appeal pending federal agencies’ release of the surprise billing final rule later this summer. The court granted HHS' request to pause proceedings while the government issues a final rule.
The ACEP, the American College of Radiology® (ACR), and the American Society of Anesthesiologists (ASA) are in favor of this hold, as the groups say they will work with CMS and other entities to ensure the final rule complies with the text and spirit of the No Surprises Act and the Texas court ruling, the ACEP said in a statement.
According to the ACEP, the groups are now pleased with the hold on the appeal and are happy that “the government is not wasting taxpayer resources to pursue its appeal of the U.S. District Court for the Eastern District of Texas decision at this time. The court's opinion affirmed that the No Surprises Act did not provide the 'give-away' to insurers enabled by the dispute resolution process published in the interim final rule.”
The original ruling sided with the Texas Medical Association, which filed a lawsuit challenging how the HHS created an arbitration process for hospitals, doctors, and insurers to settle disputes over out-of-network bills under the No Surprises Act.
The court decided that HHS was mistaken in its decision to instruct mediators to give past contracted rates between insurers and providers extra weight compared to other factors during the IDR process.
Both the Texas case and the ASA, ACEP, ACR suit impact the IDR process to determine provider reimbursement for out-of-network care. Neither case affects patient protections against out-of-network bills.
Allyson Bonner Keller, executive director of the patient connection center at Piedmont Healthcare, reflects on the use of technology to improve the patient experience and adhere to the No Surprises Act.
A poor patient financial experience can undermine an organization's reputation and the work it has put into providing the highest quality of care. A single poor registration or billing experience can negate a patients' positive, high-quality clinical experience at an organization. To avoid this, organizations must work hard to improve their patients’ overall financial experience.
Allyson Bonner Keller, FACHE, executive director of the patient connection center at Piedmont Healthcare, recently spoke at the HealthLeaders' Patient Financial Experience NOW Summit and discussed Piedmont Healthcare’s use of technology when it comes to improving the patient experience.
This transcript has been edited for clarity and length.
HealthLeaders: What technology upgrades or additions have been in place at Piedmont Healthcare to help improve the patient financial experience?
Allyson Bonner Keller: At Piedmont Healthcare patients have the use of our patient portal through our EHR vendor. It's great because we are able to connect our EHR directly into an app that is specifically for our patients.
We try very hard to create a one stop shop for our patients. We want our patients to be able to go to one app, and not only be able to schedule appointments and access the care that they need, but also see an estimate for their services. Our patients are then able to use the app to pay any co-insurance or financial liability that they have.
We have also utilized several other tools along the way to enhance the patient journey in patient financial care. Most importantly, we've used a customer relationship management tool that allows us to have scripting in place and create dedicated workflows to really guide that patient experience.
HL: What industry triggers have helped drive this focus for Piedmont?
Bonner Keller: One thing I think we can all agree on is that staffing has been a huge challenge due to the pandemic. We're all looking for how we can continue to improve our operations and be as efficient as possible without necessarily adding additional costs related to adding full-time employees.
But also, a big trigger has been the want for a digital front door. We have found that is what our patients are really looking for and it's what we've all become accustomed to, and again, I would say the pandemic only escalated this.
We've all become accustomed to having things right in front of us and available right from our phone and doing almost everything from that, so that’s really been a huge driver as well.
HL:How has the No Surprises Act affected Piedmont's need for technology when it comes to the patient financial experience?
Bonner Keller: A big component of our eligibility process and a big piece of the No Surprises Act is being able to identify an out of network plan to provide good faith estimates, so being able to utilize technology to do that has been huge for our organization.
We don't want to have someone from our revenue cycle staff have to pick up a phone, call an insurer, and then have to have a conversation with an insurance company to determine eligibility—all of that really needs to be built into whatever system you're using. In a perfect world, this would be built into the software you're using for that real-time eligibility.
We need something like this, not only for out-of-network benefits, but for in network benefits too. When it comes to gathering this information for our patients, we're only as good as the information that the payers provide back to us for real-time eligibility. Streamlining this process will only enhance our compliance with the No Surprises Act.
As a large organization with multiple sites, we also have to start thinking about how we can connect those dots across providers that maybe aren’t sharing the same EHR system or the same billing system, so if we are going to provide a holistic estimation for a patient for their services, how can we get that information and connect it into one singular estimate?
None of us want to end up after the fact with bills that we didn’t expect to receive but we have a very complex healthcare system. All of that information is hard to get to, and everyone may not want to share that information either.
Those are the hurdles we have to work through and really find the technology solutions to do that.
Again, when it comes to gathering estimates to comply with the No Surprises Act, we can’t be trying to have all of these back-and-forth conversations with all of the providers that may be involved in a patient's care, especially when that could mean three, four, or five different providers that we would be reaching out to.
The other piece that I've been focused on at Piedmont is the pre-service world—so what happens prior to that patient’s arrival? How do we provide a good faith estimate in the form that a patient wants?
Again, it's about the patient and what they want and how they can get it. All of our staff are remote now, so we can’t expect them to print out an estimate, put postage on it, and then stick it in the mail. We have to have technology solutions that help us actually get those notices out in other ways such as email or the patient portal.
But we also have to realize that there are still patients that don't have consistent internet or phone access, and not everyone is engaging in technology in the same way. Adapting our technology to improve the patient financial experience and fill these gaps and adhere to these new laws is important to us at Piedmont Healthcare and may be an ever-changing endeavor.
HealthLeaders' new series highlights five essential governing updates that cover every aspect of the revenue cycle that leaders need to know. Check back in each month for more regulatory updates.
The revenue cycle is complex, detailed, and always changing, so staying on top of regulatory updates and latest best practices requires revenue cycle leaders' constant attention in this ever-changing industry. In this revenue cycle regulatory roundup, there were an ample number of updates published by CMS and the OIG in April, including the release of the fiscal year 2023 IPPS proposed rule.
Here are the five updates you need to know.
1. There's no sign of healthcare spending slowing down as Medicare spending is projected to exceed $1 trillion in 2023.
According to CMS, although considerable uncertainty remains, the COVID-19 public health emergency (PHE) is expected to continue to influence the near-term outlook for national health spending and enrollment.
The report showed that near-term expected trends in health spending and insurance enrollments are significantly influenced by the COVID-19 PHE. It found that while there was an increased demand for patient care in 2021, the growth in national health spending slowed from 9.7% in 2020 down to 4.2% in 2021, likely as supplemental funding for public health activity and federal programs related to the COVID-19 pandemic kicked in.
The report also showed that Medicare spending growth is projected to average 7.2% between 2021 and 2030, the fastest rate of all major payers. Medicare spending is projected to exceed $1 trillion for the first time in 2023.
2. Tighten up your revenue cycle to avoid major penalties as the Office of Inspector General (OIG) takes aim at fraud.
For example, Advanced Dermatology & Skin Cancer Center (ADSCC) of Ohio, reached a $50,000 settlement agreement with the OIG to resolve allegations that offered and provided remuneration to a dermatology practice in the form of a printer cartridge, payment for holiday party expenses, and payment to a dermatology employee to prepare, pack, and complete related paperwork for specimens to be delivered to ADSCC.
Also, AltheaDX, of California, reached a settlement agreement of more than $72,000 with the OIG to resolve allegations that it violated civil monetary penalties law by submitting claims for payment for pharmacogenic tests that were not ordered by a physician.
The National Medical Services II, of Florida, reached a settlement agreement of more than $930,000 with the OIG to resolve claims that its mid-level providers fraudulently recorded personally performed services as if the services were performed by an employed physician, then improperly submitted claims for those services.
The list also included settlements to resolve allegations of violating civil monetary penalties law by employing individuals an organization knew or should have known were excluded from participation in federal healthcare programs. Those entities include River Hospital of New York, Heritage Health of Danville of Illinois, and Harney County Health District of Oregon.
3. Organizations can breathe a sigh of relief as COVID-19 PHE was renewed.
CMS continues to gradually end some emergency blanket waivers allowed under the COVID-19 PHE for some providers, but for now the 1,135 waivers remain intact for acute care and critical access hospitals.
A noticewas published announcing that the COVID-19 PHE has been extended effective April 16, 2022. This will extend the PHE and all applicable waivers tied to it for an additional 90 days.
4. CMS released the FY 2023 IPPS proposed rule and organizations are not happy.
CMS released the fiscal year (FY) 2023 IPPS proposed rule with proposals for the annual ICD-10 code update, new programs for quality reporting, and increases to hospital payment rates. Providers were not happy.
CMS projects an increase in operating payment rates by 3.2% based on a projected hospital market basket update of 3.1% reduced by a 0.4% productivity adjustment and increased by a 0.5% statutory adjustment.
"We are extremely concerned with CMS' proposed payment update of only 3.2%, given the extraordinary inflationary environment and continued labor and supply cost pressures hospitals and health systems face," Stacey Hughes, executive vice president of the American Hospital Association, said in a statement. "Even worse, hospitals would actually see a net decrease in payments from 2022 to 2023 under this proposal because of proposed cuts to disproportionate share hospital (DSH) and other payments."
Hughes continued by calling the decision "unacceptable" given that hospitals and health systems are still dealing with the COVID-19 pandemic and the variety of challenges the crisis has placed on their ability to provide patients with essential services.
5. Be on high alert: OIG announced a nationwide crackdown on healthcare-related COVID-19 fraud.
The OIG—in conjunction with the Department of Justice—published a noticeannouncing nationwide coordinated law enforcement actions to combat healthcare-related COVID-19 fraud. The action resulted in charges against 21 defendants across nine federal districts and resulted in over $149 million in false billings. Schemes involved fraudulent COVID-19 testing, billing for sham telemedicine encounters, misappropriation of Provider Relief Fund monies, and more.









36ff.jpg?itok=3VNnqk0X)



