Healthcare noncompetes are common for physicians, preventing them from working for a nearby competitor for a specific amount of time after they leave a practice.
The proposal would ban employers across healthcare and all industries from forcing noncompetes on their employees—“a widespread and often exploitative practice that suppresses wages, hampers innovation, and blocks entrepreneurs from starting new businesses,” according to a press release from the FTC.
Employers frequently use their bargaining power to compel employees across industries and job levels—from warehouse workers to healthcare executives—into signing noncompete contracts, blocking them from pursuing better opportunities, according to the FTC.
Healthcare noncompetes are common for physicians, preventing them from working for a nearby competitor for a specific amount of time after they leave a practice.
“The freedom to change jobs is core to economic liberty and to a competitive, thriving economy,” said Lina M. Khan, FTC chair.
“Noncompetes block workers from freely switching jobs, depriving them of higher wages and better working conditions, and depriving businesses of a talent pool that they need to build and expand,” she said. “By ending this practice, the FTC’s proposed rule would promote greater dynamism, innovation, and healthy competition.”
Noncompete clauses also hinder innovation and business potential by preventing entrepreneurs from forming competing businesses and inhibiting workers from bringing innovative ideas to new companies, according to the FTC.
This ultimately harms consumers because in markets with fewer new entrants and greater concentration—such as the healthcare sector—consumers can face higher prices.
The FTC’s proposed rule would generally prohibit employers from using noncompete clauses. Specifically, it would make it illegal for an employer to:
enter into or attempt to enter into a noncompete with a worker
maintain a noncompete with a worker
represent to a worker, under certain circumstances, that the worker is subject to a noncompete.
The FTC is now seeking public comment on the proposed rule, which is based on a preliminary finding that noncompete clauses constitute an unfair method of competition and therefore violate Section 5 of the Federal Trade Commission Act.
Ward's former health system had worked toward the same goal, and she found the process "transformational" and highly effective in reducing serious safety events.
Ward, who has more than 30 years of experience in healthcare administration and has served in senior nursing roles in organizations across the country, spoke with HealthLeaders about what has worked in reducing serious safety events.
This transcript has been lightly edited for brevity and clarity.
Lanie Ward, MBA, BSN, RN, is the CNO of Cambridge Health Alliance. Photo courtesy of Cambridge Health Alliance.
HealthLeaders: What are the most common patient safety issues in hospitals and health systems?
Lanie Ward: The most common patient safety issues that I see through my eyes as a CNO are [these] three: medication errors, hospital-acquired infections, and patient falls. There's no question that med errors happen with the greatest frequency. Many of them cause no harm to the patient, but some do cause severe harm and even result in patient death. That's why it's so important that we carefully evaluate all med errors, even if there was no harm.
At CHA, we put much focus on two hospital-acquired infections—catheter-associated urinary tract infections and central line-associated bloodstream infections. The frequency of these infections is much less than med errors, but they are harmful to our patients. And I must tell you that my infectious disease experts would really be upset with me if I didn't mention handwashing. That's the No. 1 one thing to prevent spreading infections patient to patient.
Patient falls are a big safety issue, and these occur everywhere, from our ambulatory clinics to our emergency departments, to our med surg-units, and even in our ICUs because some patients are more prone to falls than others.
We do find in our hospitals that patients are most at risk for falling when they're toileting—going into the bathroom, while in the bathroom, and returning to the bed—so that's why the use of purposeful rounds is so important. Purposeful rounds are proactive, frequent rounding and in those rounds we would toilet the patient.
And even though many disciplines play an important role in eliminating or reducing these patient safety issues, there's no question that nursing plays an enormous role because they're there all the time.
HL: What is one of the most effective quality improvement initiatives you've been part of to reduce serious safety events?
Ward: I feel fortunate to have been part of a health system that embarked on the journey of becoming a high-reliability organization. In my career, I found that this journey was the most transformational of any I've been involved with, and it resulted in a sharp reduction in our serious safety events. Now that I'm working at CHA, we are embarking on that same journey of becoming a high-reliability organization.
I will start by saying that the underpinning of a high-reliability organization is that there has to be a total commitment by leadership to the goal of zero harm. They have to commit to this journey financially, from a time standpoint, and to support all the staff.
Everyone in our organization received training on the principles of safety and the steps that we were going to take and the expectations of them. We took a lot of our principles from other industries—aviation and nuclear power—because those industries have been much more successful than healthcare in those areas.
There were a lot of steps in that whole journey, but the three that I thought had the most impact on reducing our serious safety events were:
1. The implementation of safety huddles
2. The expectation of speaking up for safety
3. The implementation of a just culture.
Daily safety huddles focused on patient safety issues, concerns, resolution, and follow-up, and they were implemented not only at the hospital level each day but also at the department level. In these huddles we even spoke using safety language and clarifying language so that we had the skills we need for verbal orders for handoffs, and other times that clarification was needed with communication.
Have you heard of the NATO phonetic alphabet [Alfa, Bravo, Charlie, etc.]? I would say at the huddle, "This is Lanie Ward; that's Lima Whiskey for the L and the W, and today we have 15 patients—that's one-five patients—who have indwelling Foley catheters." I found that using that language every day, and multiple times, kept the focus on all of us knowing we're doing something different. We're working on patient safety, and to be honest, it was a lot of fun. That, and the daily huddles helped us focus on patient safety at all levels.
The second was the expectation of everyone speaking up and being able to, quote "stop the line [meaning to stop a procedure in its tracks]." All of us were taught how to speak up and how to escalate it, and also how we were to respond appropriately if we were on the receiving end of someone speaking up. This training eliminated the power distance or the hierarchy between a nurse and a doctor or between a housekeeper and a nurse.
Just to give you an example of how that went, with using aviation language, a housekeeper might see a doctor walking into a room and not wash his hands. The housekeeper was expected to say, "Don't forget to wash up,"—a soft speaking up—and the physician was expected to say, "Thanks for the cross check," not "Who are you telling me to wash my hands?"
If the physician didn't respond in the way he or she was expected to, our staff were taught how to escalate and say, "For patient safety, it's important we wash our hands." If he still ignored me, then the key word was "concerned." Anyone in our organization could say, "I have a concern," and that phrase was supposed to stop the line. It really did help stop the power distance and make people feel comfortable. And they were obligated because that was our expectation.
Third, we implemented a "just culture." In the past, healthcare has held individuals accountable for all errors, and in a just culture, people are not held accountable for system failures. We had an algorithm developed that would help leaders and staff understand why a particular error occurred.
An example would be: Was the medication barcode scanning device not available, or did the nurse choose not to use it? And [that would help determine] whether it was a system problem or if we need to hold our staff accountable.
One of the things that I learned along that journey was what I call "measuring in abundance," where … I would have nurses report how many days their unit was fall-free, not how many falls they did have. It's more of a positive thing.
HL: What should nurse leaders do to help improve their organization's culture of patient safety?
Ward: It's my responsibility and all nurse leaders' responsibility to make it as easy as possible for nurses to practice safely and make it hard for them to make an error, and we need to do that by doing things like making sure we provide them with the most up-to-date modern technology; that good processes and systems are in place; that staffing is where it should be; and that their environments are conducive to safety.
Second, nurse leaders need to listen to and use the voices of the nurses who are patient-facing. We are often sitting in offices, so we need to listen.
Third, each unit should prioritize not 10 patient safety goals, but two or three based on the specifics of their unit and then identify and implement the best practices to help meet those goals.
Fourth, I talked about measuring in abundance while still looking at each incident of a fall to understand why it happened. Nurse leaders should measure abundance and celebrate, celebrate, celebrate the successes. It is so motivational for staff.
Number five, I'm a very firm believer in learning from near misses and errors that cause no harm. Don't ignore those because they could have easily gone the other way.
Finally, always remember that 'to err is human,' and support your staff. They need our support.
Innovative training program for dementia home caregivers calls for a team-based approach.
Team-centered training is the foundation of an innovative new training program designed to help home care teams solve dementia-related challenges.
ComForCare and At Your Side Home Care have launched the DementiaWise® training video series designed to change the way home care agencies approach memory care training, according to Stephanie Wierzbicka, manager of Strategic Health Programs for ComForCare.
Of the 5.8 million Americans living with Alzheimer's disease or other types of dementia, most remain in their homes as the disease progresses, which illustrates the growing need for more dementia-capable home care services.
But developing a dementia-capable workforce is challenging for the entire healthcare industry, including home care agencies. Despite traditional lecture-style training and ample care strategies, caregivers of all disciplines still struggle to apply knowledge in real-life situations, according to ComForCare.
Ineffective training and support can cause caregivers to burn out under the stress of caring for a dementia patient.
ComForCare and At Your Side Home Care, which are part of the same company, created the program to address what they believe is a design flaw that has limited traditional dementia care training: Teams often lack opportunities to plan, test, evaluate, and reflect as a team on the process of adapting responses to on-the-job challenges.
"With that problem in mind, we knew that more hours in traditional training would be inadequate to improve life for our clients, their families, and our home care teams," Wierzbicka said.
Innovative Program Design
DementiaWise doesn't just lecture the information and strategies to learners, according to ComForCare. Instead, learning about dementia care involves team-based problem-solving, reasoning, and reflection on experiences.
For example, part of the video training depicts a caregiver collaborating with her team as they encounter common dementia-related challenges in home care. By working as a unit, each team member contributes their knowledge of the disease, evidence-based care strategies, the client, and the care environment to create best-practice solutions, according to ComForCare.
ComForCare employees share real stories from their experiences to show how better solutions can be found with knowledge of dementia care, creativity, and teamwork. Indeed, the program emphasizes a process of problem-solving, not just dementia-specific content.
To understand what home care workers want and need in their dementia-care training and to assess how well the DementiaWise program addressed their needs, ComForCare and At Your Side Home Care commissioned an independent program evaluation study conducted by student and faculty researchers at Duke University Occupational Therapy Doctorate Program and Partnerships for Health, a dementia consulting company.
The odds of higher self-efficacy in ComForCare team members who watched or rewatched DementiaWise were 1.6 times the odds of higher self-efficacy than those who had not yet watched the program.
The odds of higher satisfaction in ComForCare team members who watched DementiaWise were 2.2 times the odds of higher satisfaction in those who had not yet watched it.
Participants attributed the positive outcomes to specific features of the program, including an emphasis on communication, helping clients live life to the fullest, seeing clients in their totality, and developing soft skills for caregiving on a team.
Data will be collected through November 2022, and once completed, the study’s findings will be submitted to a peer-reviewed journal and shared at a variety of professional conferences.
Cynda Rushton, PHD, MSN, RN, the Anne and George L. Bunting Professor of Clinical Ethics at Johns Hopkins, is the study’s principal investigator and agreed to a short Q&A about the study. Her answers have been lightly edited for brevity and clarity.
HealthLeaders: Besides an event like the COVID-19 pandemic, what are the types of crisis situations this study might address?
Cynda Rushton: This study aims to understand the range of ethical challenges that nurse leaders faced during the pandemic. Some are specifically related to the pandemic and others are longstanding issues that nurse leaders have faced that were exacerbated by the pandemic.
HL: What is an example or two of ethical concerns that a nurse leader might face during a crisis?
Rushton: Allocation of scarce resources, including human resources (staff), in a way that is equitable, respectful, and fair to both the employees and the people they serve. During the pandemic, many nurse leaders were involved in determining who would be able to be present with patients including at the end of their lives and they struggled to make consistent and fair decisions.
Nurse leaders were responsible for budgetary decisions that involved unacceptable tradeoffs or dealing with the pay inequities created by needing to use temporary traveling nurses to meet patient needs.
HL: Can you provide an example of what a couple of the questions are on this survey?
Rushton: The questions focus on key issues that nurse leaders may have faced, their appraisal of organizational effectiveness in responding to them and how the challenges impacted them.
True flexibility starts with recognizing that 'flexibility is much more than the option to choose the location one works from.'
Flexible work is here to stay, yet there are drastic differences in the way women and men experience flexibility the workplace, a new study says.
While men are significantly more satisfied with the flexibility that their workplace offers, women indicate their workplace is less supportive of their flexibility needs, which are not being met, according to research by Werklabs, the research division of The Mom Project, a platform for supporting the economic advancement of working mothers.
Clear demographic differences arose regarding male and female respondents. Women, who viewed themselves as the primary caretaker in their families, expressed a higher need for flexible hours and days of work, owing to needs such as attending to family appointments, picking up children from school, and being able to respond to last-minute needs.
Managerial support for flexibility is helpful for women, but it is not enough, as many are reluctant to be perceived as receiving special treatment or less committed to their careers, according to the research, which involved surveys of more than 1,700 full- and part-time workers to gather data.
One research participant explained: "While we now work in a hybrid model, I have to request and explain why I need to only work two days in office even though I'm willing to work four days … the following week. There is rigidity in what is supposed to be a hybrid work arrangement."
True flexibility, rather than prescribed flexible "benefits," must become part of an organization’s DNA, said the study. True flexibility starts with acknowledging that “flexibility is much more than the option to choose the location one works from; true flexibility includes key traits such as the autonomy to get the job done on one's own terms and flexible working hours during the day and across the work week, among others,” the study says.
Without true flexibility, women are significantly less likely than men to recommend their current employer to others as a compassionate place to work, anticipate an increase in their productivity, or remain with their current employer at all, the research indicates.
"The reluctance of women to take advantage of flexibility in the workplaces or advocate for their needs reflects long-standing biases against working women, particularly working mothers,” said Pam Cohen, PhD, chief research and analytics officer at WerkLabs.
“This study highlights the incredible importance of corporate cultures and managers truly understanding the needs of working moms and actively giving women permission to exercise flexibility so they can bring their fullest selves to work, and contribute to closing the gender pay gap,” she said.
The research identified six factors in creating true flexibility:
Organizational support: the degree to which employees believe their organization values their work contributions and cares for their wellbeing through flexibility
Personal autonomy: the degree to which employees are empowered to make choices about where and when they work, defining flexibility on their own terms
Managerial support: the role in which managers play in establishing flexibility through practice
Paid time off: the sense employees feel they have a reasonable number of PTO to accommodate both their own and their family’s needs
Workload: how manageable, supported, equitable and consistent employees’ workload is
Team support: the ways immediate colleagues contribute to a culture of flexibility
Many employers still don’t understand the subtleties of flexibility at work and how to implement practical changes so that they may see progress toward building more flexible work structures, the study says.
“A coordinated focus on organizational support and personal autonomy,” it concludes, “highlights significant opportunities for consequential change in the workplace.”
The Kindness Initiative has changed the culture as it’s expanded throughout the Northside Hospital System.
Carolyn Booker, DNP, RN, NEA-BC, chief nursing officer of Northside Hospital Forsyth, in Cumming, Georgia, was troubled how violence was making its way into places she considered to be sacred and safe: schools, churches, and hospitals.
Kindness, she thought, could be an antidote, so in 2018 she began exploring the possibility and ultimately developed The Kindness Initiative, which has caught on and rippled through all of Northside’s campuses.
HealthLeaders spoke with Booker about how The Kindness Initiative was developed, why it has taken off like wildfire, and how it has changed the health system’s culture.
This transcript has been lightly edited for brevity and clarity.
HealthLeaders: How did The Kindness Initiative originate?
Carolyn Booker: What I began to see in the media was that there did not seem to be any protection against violence. That level of negativity happening out in the world was making its way into the hospital setting, and I wanted to figure out a way to address that. I began to look at the whole concept of kindness, just a Google search, and saw the effects of being kind and then I got the idea to do something.
The definition of kindness I like to use is the one that points to the fact that it's when you do something for someone just to make them feel better, with no expectation of anything in return. This was around the holidays, and we had gotten this huge basket of candy at the hospital. I took that basket and went over to labor and delivery, sat it at the nurses’ station, and said, “Guys, this is for you.” The reaction that came from that unexpected act just gave me a buzz.
I did more research and found an organization called kindness.org, which promotes kindness, and found they had these kindness toolkits. Our Kindness Initiative got started because of this thought about how we could possibly take kindness and make it the norm within the hospital setting.
HL: How did The Kindness Initiative begin to spread throughout the hospital?
Booker: I have a series of meetings with employees, and I began to bring this Kindness Initiative into the work environment and started talking through it and sharing YouTube videos of acts of kindness that people were demonstrating for others. The impact of it—people seeing that versus all this negativity—was extremely huge.
I got the idea to do the Kindness Challenge in November 2018, which was spurred by kindness.org, in which we would challenge employees to log acts of kindness. These acts could be in their community, in their home, or it could be at work, and they had to log and submit 12 acts of kindness, because we were counting them up. The goal was to have 10,000 acts of kindness by May 11.
When a person submitted their 12 acts of kindness, we would give them a T-shirt, and that component turned out to be almost like cultural iconography. It was a gray T-shirt that had white lettering and black lettering on it with a red heart and it said, “You have a choice. Choose kindness. I did.” We had to order three times to keep up with the acts that were being submitted.
By May 11, we had more than 11,000 acts of kindness that we had logged in terms of our employees, and those things were not necessarily huge things because we wanted any act of kindness—acknowledging one another, making eye contact, speaking to each other, and seeing each other because that's something that's important as well. The whole environment was positively charged because of this particular activity.
HL: Why do you think it took off and spread so quickly?
Booker: Because it came out of leadership. Every month, we had the Patient Care Council, and a part of that meeting would involve leaders going out to the different units and talking to staff, asking them about their work experience. And then we would ask them, “If there was someone here that you could recognize who would that be?” Then, the leaders would go and find that person and share what their colleague had said about them.
Again, the kindness made a huge difference. It was the talk of the organization at that time. It was very powerful, and we went on to take kindness and just interweave it into everything.
HL: How has The Kindness Initiative changed the culture at Northside?
Booker: This initiative is now a part of the Northside Hospital system. It is not just here at Northside Forsyth; it is across the system. We have a systemwide team—the Kindness Through Communication team—that meets every week to work on ways to embed kindness into the organization’s culture.
Northside has engaged an organization that has created a program called Excellence in Action for peer and leader recognition. This system is similar to Facebook, but it's an internal Facebook, so there is a livestream of this recognition on our intranet.
Another thing we've done as an organization is that all our service standards contain kind elements, which includes supporting co-workers, the ways in which we demonstrate kindness toward our patients, and ways we can be fiscally responsible and kind to our work environment.
HL: What has data shown about The Kindness Initiative?
Booker: It’s like anything else; you wax and you wane. Our patient experience scores reflect the fact that patients recognize when staff members are kind. The other thing that happens when you have kindness that resounds within the organization is that you have very good scores from the standpoint of your externally reported metrics.
HL: And those scores have gone up; is that what you're saying?
Booker: They go up, they go down, then they go back up, because of the fact that it's reflective of life.
HL: How can other nurse leaders begin to implement something like The Kindness Initiative in their hospital?
Booker: Look at the literature because it’s proliferative. Dignity Health on the West Coast is a hospital system that is doing a phenomenal job with kindness, along with the University of California, Davis. They do a phenomenal amount of research on the effects of kindness and the effects of mindfulness, because those things go together.
While it has not translated itself to the masses in the ways that a lot of other things have gone viral, I would expect that, with concentrated effort, we could get there.
Nursing students were left hanging in the middle of their school year when Stratford University closed down.
More than 350 nursing students left hanging when Virginia-based Stratford University closed its doors September 30 will be able to continue their education through Chamberlain University.
Chamberlain, which has the largest school of nursing in the United States, has entered into an agreement with Stratford that will allow the displaced nursing students to transfer to Chamberlain’s Tysons Corner, Virginia, campus or choose the BSN Degree Online option, according to a press release issued by Chamberlain.
Stratford closed all its campuses in Virginia and Maryland at the end of the fall term after announcing late last month that it was shutting down amid financial issues and an apparent dispute with the U.S. Department of Education. Students were given just one week’s notice of the closure.
“Chamberlain will accept students who meet the university’s admission requirements so they can work toward completing their nursing degrees and contribute to the nursing workforce which desperately needs more nurses,” according to the university. “After a comprehensive mapping of curriculums, Chamberlain can accept a generous amount of Stratford BSN credits eligible for transfer.”
Former Stratford students who apply and are accepted to Chamberlain can enroll as soon as the November 2022 session or have the option to begin with January and March 2023 sessions for Tysons Corner campus or BSN online.
“We are glad to be located near the Stratford University campuses so we can help these displaced students continue their nursing education and dream of becoming a nurse,” said Lindsey Bradbury, MBA, BSN, RN, Tysons Corner campus president.
Indeed, not only is Chamberlain planning webinars, on-site meeting opportunities, and tours of the Tysons Corner campus to help interested students learn more about Chamberlain, but it is waiving application fees and expediting applications for Stratford transfer students so they can start at the November session.
“As an experienced nurse and leader of Chamberlain, I know first-hand the challenges nursing students face, such as intense studying, exhausting clinicals, and some even working full-time, and we are glad to help these aspiring nurses complete their degrees,” said Karen Cox, PhD, RN, FACHE, FAAN, president, Chamberlain University.
“Chamberlain recognizes the critical shortage of nurses we have in the U.S.,” Cox said, “and we do everything we can to support our students and hope our Chamberlain Care® values provide an extraordinary nursing education for these students and will encourage them as graduates to go on to make an impact on healthcare around the world.”
The plan: To advance equity and improve healthcare workforce diversity by training people from historically marginalized and underrepresented populations.
Nurse training programs are getting $80 million from the U.S. Department of Labor to expand the pipeline and get more nurses into short-staffed healthcare centers.
The Nursing Expansion Grant Program also will advance equity and improve healthcare workforce diversity by training people from historically marginalized and underrepresented populations, according to the department’s press release.
The funding comes not a moment too soon, as the U.S. Bureau of Labor Statistics projects that more than 275,000 additional nurses are needed from 2020 to 2030, and that employment opportunities for nurses will grow at 9%—faster than all other occupations from 2016 through 2026.
“The funding opportunity … will support training and other programs to help advance workforce equity while bringing more nurses into the industry,” said Secretary of Labor Marty Walsh.
These H-1B Skills Training Grants will be administered by the department’s Employment and Training Administration and will address bottlenecks in training the nursing workforce while expanding and diversifying the pipeline of qualified nursing professionals through two training tracks.
The first track—the Nurse Education Professional Track—will increase the number of clinical and vocational nursing instructors and educators by training new or upskilling experienced current or former nurses, including retired nurses, into advanced postsecondary credentialing.
The second track—the Nursing Career Pathway Track—will train frontline healthcare professionals and paraprofessionals, including direct care workers, to advance along a career pathway and attain postsecondary credentials needed for middle- to high-skilled nursing occupations during the grant period of performance.
Applicants for the second track will propose strategies to improve nursing professional, clinical instructor, and educator recruitment, preparation, development, training, and retention.
Applicants must propose training program models that attract workers, unions, worker organizations and employers while building partnerships with community-based organizations and training institutions, according to the labor department.
Violence in the emergency department not only poses a threat to employees, but it harms patient care, doctors say.
Assaults in the emergency department are on the rise with nearly one-fourth (24%) of emergency physicians reporting being assaulted multiple times a week,according to the findings of a new poll from the American College of Emergency Physicians (ACEP).
Indeed, 85% of emergency physicians believe the rate of violence in their department has increased over the past five years, primarily by patients and patients’ family members.
Their nursing colleagues will agree. More than 5,000 nurses were assaulted on the job in the second quarter of 2022 alone, according to shocking new data from Press Ganey.
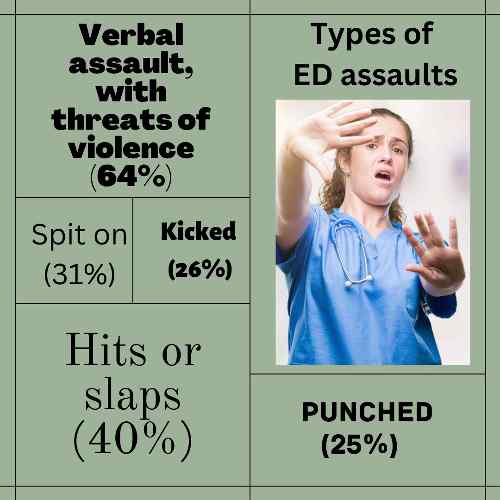
The most common types of assaults, according to the new poll, are:
Verbal assault, with threats of violence (64%)
Hits or slaps (40%)
Spit on (31%)
Kicked (26%)
Punched (25%)
Those most often responsible for assaults are psychiatric patients (42%) and those seeking drugs or under the influence of drugs or alcohol (40%), the poll says.
“I've been scared for my safety as well as the safety of my family,” he said. “I once had a patient's family member with a gun holster on his hip threaten to kill me and my entire family after I told his father that he needed to be admitted because he had coronavirus.”
Skog also told of overhearing an inpatient unit nurse who came to help the busy emergency department say to another nurse, “I'm telling my supervisor that I'm never coming down here to help out again. This is just not safe.”
No consequences has consequences
Much of the rise of violence in hospitals since 2018 has been caused by a lack of punishment, the poll indicates. Only 2% of hospital security pressed charges. The most common responses are escorting the patient out of the facility, restraining the patient, or no action at all.
“It depends on the hospital as well as the state where the hospital is located,” said Chris Kang, MD, FACEP, president-elect of ACEP. “Where I work, in Washington state, requires hospitals to have a prevention plan.”
Some hospitals simply don’t want to proceed with charges; other times, law enforcement does not follow up, Kang said.
Such violence affects patient care, the study shows. For example, among emergency physicians polled:
89% agree violence in the emergency department harms patient care, a 12% increase from 2018.
85% say ED violence has resulted in an increase in wait times.
60% report these attacks often result in patients leaving the emergency department without being seen or treated by a doctor.
87% report a loss of productivity from the physician or staff as a result.
85% report emotional trauma and an increase in anxiety because of ED violence.
Working for change
Emergency physicians are counting on hospitals and legislative bodies to provide protection against violence, Skog said.
Some hospitals have taken steps to protect their employees and patients from violent outbursts, such as Maine Medical Center in Portland, Maine, which has increased security guards, locked down some doors, and installed metal detectors at main entrances and at the ambulance entrance.
And when an altercation—verbal or physical—begins at Inova hospitals, it is quickly met with a rapid-response team specially trained to de-escalate and safely contain the fracas.
ACEP and the Emergency Nurses Association launched the No Silence on ED Violence campaign in 2019 to raise awareness, advocate for policy changes on the state and federal level, and strengthen protections for frontline workers.
The emergency physicians’ group pointed to federal legislation that could bolster protections for healthcare workers.
The bipartisan Safety From Violence for Healthcare Employees (SAVE) Act, introduced to the U.S. House of Representatives in June, would criminalize assault and intimidation of healthcare workers.
The U.S. Senate is considering legislation—the Workplace Violence Prevention for Health Care and Social Service Workers Act—requiring healthcare and social service sectors to develop and implement workplace violence prevention plans.
“Emergency medicine is hemorrhaging nurses, technicians, and doctors that rightfully can no longer accept the ongoing violence that they experience daily,” Skog said.
“Now, more than ever, I fear that we will lose these frontline medical professionals unless action to increase accountability and add protection in the emergency department is addressed with the seriousness and urgency required to stem the tide of violence."
Funding intends to create more faculty positions and increase student graduation and placement rates.
Nursing schools at 11 colleges and universities in New Mexico received a portion of $30 million in faculty endowments from the New Mexico Higher Education Department to recruit and retain faculty and other supports.
The greatest share—$6.5 million—will go to theUniversity of New Mexico’s Health Sciences Center to fund at least three additional nursing faculty to conduct research and prepare graduate students to enter leadership and faculty roles in healthcare and nurse education.
The university’s College of Nursing has the state’s only nursing PhD program and produces nurse educators for New Mexico’s 18 other public nursing programs, according to a press release from the state’s Higher Education Department.
The nurse funding is part of a larger $110.5 million endowment spread over 13 colleges and universities. Educator preparation programs will receive $50 million, and social work programs will receive $30.5 million, also to recruit and retain faculty.
“This funding will enhance our ability to attract and keep talented faculty to grow and sustain the pipeline of licensed educators, nurses, and social workers that support the lifelong success, health and well-being of New Mexicans,” Gov. Michelle Lujan Grisham said. "These are critical fields that are experiencing workforce shortages around the country, and this administration is committed to doing whatever is necessary to build up our in-state pipeline."
The millions are invested to generate revenue year after year that fund faculty positions, support internships and residencies, and finance other activities to increase graduation and placement rates of students in relevant career fields.
Nursing schools at these colleges and universities received funding:
The University of New Mexico’s Health Sciences Center—$6.5 million
Central New Mexico Community College—$3 million
New Mexico Highlands University—$2.5 million
The University of New Mexico–Gallup—$2.5 million
New Mexico State University—$2.5 million
Doña Ana Community College—$2.5 million
Northern New Mexico College—$2.5 million
Mesalands Community College—$2 million
Santa Fe Community College—$2 million
Western New Mexico University—$2 million
San Juan College—$2 million
“The $2 million endowment funds for nursing faculty stipends at Santa Fe Community College is critical to meet the demand for expanding nursing education in the region,” said Terri Tewart, the college’s dean of Sciences, Health, and Engineering and Math.
“This endowment will make it possible to accept eight to 16 more students into our nursing program. Santa Fe Community College is expanding our faculty with one full-time and another part-time nurse educator,” she said. “We are incredibly grateful to the New Mexico Higher Education Department and the New Mexico Nurses Association for working on the pathway for this grant funding.”



_resize.jpg)








.jpg?itok=Vj-UrfWD)