A new personal protective equipment manufacturing company is set to open in Cincinnati next year.
Bon Secours Mercy Health has established a strategic relationship with a locally based manufacturer of personal protective equipment (PPE).
Securing supplies of PPE was one of the most challenging healthcare supply chain challenges of the coronavirus pandemic. In the United States, reliance on foreign suppliers of PPE such as China-based manufacturers led to shortages.
Cincinnati-based Bon Secours Mercy Health has forged a strategic relationship with Emerge Manufacturing, which is building a 50,000-square-foot facility in the Roselawn-Bond Hill neighborhood of Cincinnati. Emerge was founded by Cynthia Booth, a Cincinnati business leader and entrepreneur.
"We are excited to work with someone like Cynthia who has advanced thinking. She is all about the community. She is all about how we can bring to life not only local jobs but also a solution for a global supply challenge," Daniel Hurry, MBA, chief supply chain officer at Bon Secours Mercy Health and president of Advantus Health Partners, told HealthLeaders.
Advantus is a subsidiary of Bon Secours Mercy Health that specializes in supply chain functions. "We put up our own supply chain organization so we could do things more strategically, effectively, and efficiently rather than relying on third party resources that might be in a traditional group purchasing organization model," Hurry says.
Emerge plans to manufacture face masks, surgical masks, N95 masks, clinical gowns, and other PPE. Construction of the company's manufacturing plant is slated to begin in the first quarter of 2023, with an expected opening in early 2024.
Bon Secours Mercy Health has invested in Emerge, Hurry says. "We made a meaningful and significant investment. All the way from the start, we were talking about how to support Cynthia in making sure that we have resiliency in how we supply while supporting local communities. While there is a monetary investment, there is also strategic investment in helping to support and develop the relationship."
He declined to specify the amount of the financial investment.
The strategic relationship is focused on gauging the PPE market, Hurry says. "It is important that we are keeping an eye on the challenges that are in the market. We are looking at raw material factors. We are looking at logistics challenges. We are looking at what may need to be addressed in the future rather than what may have been a pinch point historically. It is no secret that masks and gowns were the highlight of the challenge historically. That does not mean that will be in the challenge in two or three years—it may be something else. Strategically, we want to have continuous dialogue and continuous engagement."
Advantages of domestic supplier of PPE
For Bon Secours Mercy Health, there are several advantages to having a strategic relationship with Emerge, he says. "An advantage is the direct connection on the full manufacturing process. It creates jobs locally. It creates jobs domestically. It keeps us aligned with what the market can bear in this particular product mix."
Having domestic sources of PPE is crucial for U.S. healthcare providers, Hurry says. "It is critically important to have a resilient portfolio that is not contingent upon a region of the globe. If you have shutdowns in plants overseas and they cannot produce or move product, you run into challenges where it does not matter what your logistics model is—there is nothing to move."
PPE is an essential supply category for healthcare providers, he says. "With PPE, we forget to talk about what it is. Personal protective equipment protects people from disease and the risk that comes with it. With those types of products, resiliency becomes even more important than many other products. When there are elective products, you still need resiliency but the risks at hand are not quite as dramatic if you cannot protect people on an ongoing basis."
With a shortage of nurses, Memorial is relying on traveling nurses, which is placing a financial strain on the health system.
Nursing shortages are having a significant impact on Memorial Healthcare System, according to Marc Napp, MD, MS, executive vice president and chief medical officer of the health system.
Napp has served as Memorial's CMO since March 2021, succeeding Stanley Marks, MD, who retired in late 2020. He previously served as deputy chief medical officer at Mount Sinai Health System in New York. Before working at Mount Sinai, he served in medical leadership roles at Northwell Health in New York.
HealthLeaders recently discussed a range of issues with Napp, including workforce shortages, physician burnout, and clinical care predictions for 2023. The following transcript of that conversation has been edited for clarity and brevity.
HealthLeaders: What are the primary challenges of serving as the CMO of Memorial?
Marc Napp: The biggest challenge is the workforce—primarily nursing. We have had to bring in many nursing travelers from outside the organization, which can dilute the culture. When you bring in people from the outside, it is difficult to inculcate them overnight. There is also concern about the stability of the workforce because people are coming and going.
Another challenge is getting back on our feet after going through the coronavirus pandemic and the financial impact that the pandemic has had on us. With an itinerate workforce and the premium price that it costs, it puts a lot of our capital investments at risk because there is only so much money in the budget. We are spending a premium on our labor. While our hospitals are full and our emergency departments and operating rooms are busy, the cost to deliver care is significant and it is making it difficult to operationalize some of our plans.
HL: How are you rising to these challenges?
Napp: Fortunately, we have a very substantial bank account, so we can weather the storm—at least for the short-term and the medium-term. But we do not want to use our reserves for operations, and the portfolio took a hit when the market took a hit. Right now, we are managing our challenges because we have money in the bank. However, at some point, we are going to have to make some hard decisions. We are working on cost containment. We are cutting back on the premium labor, and we are growing certain programs that we had planned on growing before the pandemic hit.
If you were to look at us from the outside, you would not necessarily notice that there is any issue, unlike some of the other organizations across the country that are reporting massive losses. We are having losses, but they are not massive. So, we can hold our own for now.
Marc Napp, MD, MS, executive vice president and chief medical officer of Memorial Healthcare System. Photo courtesy of Memorial Healthcare System.
HL: What is the status of physician burnout at Memorial?
Napp: I must give the care providers at Memorial some credit. Their fortitude and their resilience have been impressive. We have lost few physicians to retirement or career changes as a result of the pandemic or burnout. There has been an impact on morale and work ethic to a degree as it is affecting every health system, but I have been impressed with the resilience of this group. We are concerned about wellness and burnout. But as far as burnout goes, I am aware of it and we are addressing it, but it has not been demonstrated to be a major concern for us at this point.
HL: How is the health system coping with physician burnout?
Napp: One thing I have noticed about Memorial compared to other organizations is that this is a place where people really love to work. We do a physician engagement survey every two years and we are going to start doing it annually. We are top decile in the country in terms of physician engagement. People like to work here. They are proud of working here. They feel supported, and like the organization cares about them, and that goes a long way in dealing with a lot of the burnout issues that other organizations are seeing.
In general, we have very little physician turnover, which is one measure of burnout. Part of that is the respect that the staff has for physicians and the mutual respect that physicians have for the staff. It is a collegial environment. There is tremendous rapport between the nursing staff and the physician staff. When you go to a small-town community hospital, it feels intimate, warm, and inviting. Despite the fact that we are a six-hospital system, you get the same feeling when you are in our facilities. That goes a long way to addressing the burnout issues that you see at other health systems.
Another thing that is important is there is respect for physician leadership at Memorial. We do a lot to support our medical staff leaders. The medical executive committee at this organization feels like they do something. At every other place I have been, the MEC wonders why it even bothers meeting. At Memorial, the MEC has a significant role to play. The medical staff officers are actively involved in what goes on in the hospitals. I am grateful to them because I have a great set of physician officers.
HL: Do you have predictions for clinical care in 2023?
Napp: We are going to see a rapid return to the way we used to do business before the pandemic. We are going to see some decline of telehealth, although there will be places where telehealth continues to make sense.
There will also be some significant innovation because we learned that we could innovate during the pandemic—we had to solve problems on the fly and remote patient monitoring is an example of that innovation.
We are going to see more of the same issues that plagued us before the pandemic in terms of difficulty discharging patients because of lack of placement opportunities in the community, complexity of the payment system, and issues of people not being able to access care. We haven't fixed many of the issues that existed before the pandemic—they just became less important in the scheme of things over the past two-and-a-half years. So, these issues are all going to resurface, and I am concerned about people feeling frustrated by these issues because we had some workarounds during the pandemic that made life easier that are not going to be there in the future.
HL: What are your primary challenges now that the crisis phase of the pandemic has passed?
Napp: What has happened in our area is clinical, but it is also operational and business-related. The certificate-of-need mandates were lifted in Florida, and we are a safety net health system surrounded by for-profit and aggressive not-for-profit health systems that are not safety nets. So, we take care of everybody whether they have an ability to pay or not. We have programs in place specifically for people who do not have insurance. We are taking care of those people, but that comes off our operations budget.
What is happening with the lifting of the certificate-of-need requirements is more competition, which is generally a good thing because it drives better performance, but it is not fair when the playing field is not level. I am concerned about skimming of patients—other health systems are getting the well-paying patients and we are being left holding the bag for the uninsured or poorly insured patients.
HL: How would you describe your leadership style?
Napp: I am collaborative. I feel strongly that I need to promote people to be experts in their areas and to recognize their expertise. So, I don't tend to be dictatorial or directive. That can lead to slower decision-making, but I do find that in the long run it has been the most successful way for me to lead. I am most comfortable in that mode.
The only time I lead in a different way is when we have a crisis situation such as an emergency management role. In that case, I become more directive. But even then, there is always going to be a cabinet of people I listen to. I am fortunate—I have some great leaders that I work with who have tremendous expertise, and I rely on them for counsel and to figure out what is best for the organization.
Learn about healthcare worker burnout research and methods for addressing burnout at your organization.
With the coronavirus pandemic in its third year, healthcare worker burnout was a top concern in 2022. The following seven HealthLeaders stories provided insight and solutions for healthcare worker burnout.
This article appeared in the November/December 2022 edition of HealthLeaders magazine. Health systems and hospitals realize a return on investment when investing in the wellness of the clinical workforce. Learn about how to address burnout among physicians and nurses.
The physician burnout level and other measures of physician distress increased dramatically during the pandemic, a research article found. In survey data, mean emotional exhaustion scores among physicians increased 38.6% from 2020 to 2021.
Nearly 32% of nurses planned to retire or leave the field altogether, while 40% planned to pursue a nursing role elsewhere, a study found. Nearly half of nurses surveyed said they planned to change jobs because of burnout and a high-stress environment.
In survey data, emotional exhaustion among physicians decreased from 31.8% in 2019 to 28.3% in 2020, then increased to 37.8% in the second year of the pandemic. Emotional exhaustion among nurses increased from 40.6% in 2019 to 46.5% in 2020 and 49.2% in the second year of the pandemic.
The American Nurses Association partnered with SE Healthcare to create the Burnout Prevention Enrichment Center. The web-based platform offered 24/7 access to a collection of tools and audio and video educational content to help prevent career burnout.
Survey data showed that 45% of clinicians reported burnout in 2019, with the burnout rate rising to 60% in late 2021. Higher rates of burnout were reported in chaotic workplaces (odds ratio 1.51) and settings with low work control (odds ratio 2.10).
At Bon Secours Mercy Health, a peer support program is a key component of the health system's healthcare worker well-being efforts. Bon Secours Mercy Health's peer support program started with physicians in May 2020 and has grown to serve all healthcare workers.
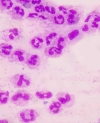
Sepsis can develop as the result of any kind of infection, including influenza.
Influenza patients are at risk of developing sepsis, according to the Sepsis Alliance.
Sepsis is the body's extreme reaction to an infection, and it can lead to tissue damage, organ failure, and death, according to the Centers for Diseases Control and Prevention. CDC annual statistics on sepsis are eye-popping: about 1.7 million American adults develop sepsis, at least 350,000 American adults with sepsis die during their hospitalization or are discharged to hospice, and 1 of 3 people who die in a hospital had sepsis during their hospitalization.
There are two primary connections between sepsis and influenza, says Jim O'Brien, MD, MS, vice president of operations for population health at OhioHealth and a member of the Sepsis Alliance Board of Directors.
"First of all, sepsis can be caused by any sort of infection, including influenza. Sepsis can be viewed as an inappropriate response to an infection. So, viral infections can lead to sepsis as much as bacterial infections, fungal infections, or even parasitic infections. There also is a secondary connection that occurs. It is relatively common for people who get severely ill with influenza to also be at higher risk of developing a secondary infection with a bacteria—in particular, bacterial pneumonia. So, patients may end up with influenza and particularly influenza pneumonia, then subsequently develop a bacterial infection that can lead to sepsis," he says.
Sepsis is the cause of death for many influenza patients, O'Brien says. "Annually, there about 200,000 hospitalizations that are associated with influenza, and there are around 40,000 deaths. If you look within those deaths, there is a significant number of patients who end up dying of sepsis, either associated with the influenza or a bacterial infection."
It can be difficult to diagnose sepsis in influenza patients, he says.
"The good news with influenza is we have good diagnostics for determining whether someone has influenza. The challenge that we have is isolating the people who feel terrible with influenza versus someone who subsequently develops organ failure and sepsis, where they are at higher risk of dying. It gets tough when people ask, 'When should I know to go see a doctor?' We talk about having an elevated temperature due to sepsis, but influenza can result in a temperature of 103 in adults. A high temperature does not necessarily mean you are developing sepsis. Generally, we talk about if patients are feeling the worst they have ever felt; but for young and healthy people, those symptoms can be driven by influenza."
Changes of cognitive status in influenza patients can indicate the development of sepsis, O'Brien says. "One of the big triggers in influenza patients that indicates the development of sepsis is if someone's brain is not working the way it should be working. You may not be able to wake the patient. They may be confused. Those are real warning signs of someone who has developed complications beyond just feeling terrible with influenza, and they should seek help."
There also are risk factors for sepsis in influenza patients, he says.
"Extremes of age are a risk factor—children under 5 and adults over 65. Those extremes are at much higher risk for influenza complications, including sepsis. The farther you get to the age extremes, the higher the risk of sepsis. So, children less than 2 are at greater risk than children less than 5, and adults over 80 are at greater risk than adults over 65. Pregnant women with influenza are at risk of developing sepsis—there are certain races and ethnicities of pregnant women who are at higher risk of developing sepsis. It appears that Native Americans and Alaskan Natives are at higher risk of complications from influenza such as sepsis compared to White populations. Influenza patients with chronic medical conditions such as diseases that affect the immune system are at higher risk for sepsis. People who live in long-term nursing facilities or skilled nursing facilities are other people that we worry about."
The best way to prevent sepsis in the context of influenza is to get a flu shot, O'Brien says. "Flu shots are not perfect, but they are the best form of protection against severe disease from influenza, including sepsis. If you look at patients who progress enough that they need to be on a ventilator, people who did not get vaccinated are six times more likely to be on a ventilator from influenza than those people who got vaccinated. So, flu shots are the first line of defense."
Taking measures that prevent the spread of infection are also important to avoid sepsis developing from influenza, he says. "Washing hands frequently is helpful. Covering our mouths when we sneeze or cough is helpful. If we are sick, not being around other people is helpful. Those measures work."
The Sepsis Alliance offers resources on influenza and sepsis, including a sepsis and fluwebpage that features infographics and information guides as well as a free webinar for healthcare professionals.
AdventHealth's Neil Finkler predicts healthcare workforce shortages will spur adoption of technology such as artificial intelligence and machine learning.
The shift of medical services from the hospital setting to the ambulatory setting and the home will accelerate in 2023, the chief clinical officer of AdventHealth's Central Florida Division predicts.
Neil Finkler, MD, became AdventHealth's chief clinical officer for the six-county region in 2021. In 1992, he joined AdventHealth Orlando, where he founded the gynecologic oncology program and fellowship program. Before taking on his current role, he was senior vice president and chief medical officer for AdventHealth Orlando's acute care services.
HealthLeaders recently talked with Finkler about a range of issues, including clinical care predictions for 2023, the challenges he faces as a chief clinical officer, physician burnout, and workforce shortages. The transcript of that conversation below has been edited for brevity and clarity.
HealthLeaders: What predictions do you have for clinical care in 2023?
Neil Finkler: We will continue to see an out-migration of hospital-based procedures that are transitioning to outpatient settings, specifically ambulatory surgery centers.
The hospital at home models will continue to grow nationwide next year. Health systems are looking at how they can care for chronic conditions in the home. They are also looking at identifying the triggers when a patient is in trouble at home, and they are looking at how they get the appropriate care at home. If you think about populations at risk, where we as healthcare providers will be at full risk, we need to put the appropriate patient in the appropriate setting at the appropriate time. The least costly setting remains taking care of the patient at home. Many health systems have been dabbling with hospital at home, and we will see more innovative and creative models as we move forward.
Another thing we are going to see, and we are beginning to see it in the post-pandemic world, is that the nontraditional healthcare players including retailers such as Walmart and the Amazons of the world are going to start expanding beyond what they have done in healthcare so far. We are going to see them do blood tests, vaccinations, and other medical services that have traditionally been delivered in the hospital setting.
In our market, Walmart has been opening health clinics. They have behavioral health. They are adding ophthalmologic services, and they are putting services in one easy place for the consumer and making it an affordable option.
We are also going to see a continued look at how we leverage technology to automate tasks to alleviate our workforce restraints. This includes artificial intelligence, machine learning, and remote monitoring. For example, we can use this technology to determine who is at risk for a readmission after a coronary bypass.
We can use artificial intelligence and machine learning to help us identify whom we need to put resources around once they get discharged, so that their readmission rates are lower and their utilization rates in the emergency department are lower, which will give us more inpatient capacity.
Neil Finkler, MD, chief clinical officer of AdventHealth's Central Florida Division. Photo courtesy of AdventHealth.
HL: What are the primary challenges of serving as the chief clinical officer of the Central Florida Division of AdventHealth?
Finkler: Before the pandemic, we were clearly on a pathway of top performance and performance improvement from a quality standpoint. Our organization defines clinical excellence as being a Centers for Medicare & Medicaid Services 5-star and Leapfrog A. We had achieved those goals in the early days of the pandemic, but we have slipped, particularly in the CMS star rating—we were a 5 star and now we are a 4 star.
This slippage has clearly been created by the pandemic, with things like workforce shortages, burnout, some financial instability, and supply chain constraints. All of this has shifted our focus and made it harder to keep up with the processes that we know are needed to maintain top quality and safety. One of the things we are doing as we emerge from the pandemic is putting our efforts back on those processes that we know work so we can get back to a CMS 5-star rating. The particular areas that we struggle with are hospital-acquired infections as well as readmissions.
Another challenge that we have is the workforce. As we look forward into the future, we know that our population here is growing and we know that the population in Central Florida is aging. In addition, chronic diseases such as diabetes, chronic obstructive pulmonary disease, and cardiovascular disease continue to increase. This increase in demand for healthcare services while we experience workforce shortages is going to challenge us.
Another challenge is the value transformation, where we are looking to improve the value proposition for both patients and payers. The question is, how do we improve quality while decreasing cost? Both the payers and the patients continue to expect reductions in waste and for us to cut the costs of healthcare.
HL: What is the status of physician burnout at AdventHealth?
Finkler: It clearly exists. Our workforce, not just physicians but also our nursing workforce and other members of the clinical workforce, has not yet fully recovered from the impact of the pandemic. Burnout remains prevalent, in many cases unrecognized. Even though COVID-19 admissions have decreased, the hospitals are still full and the clinical demand on our physicians continues at an all-time high. All of this contributes to physician burnout and dissatisfaction.
What are we doing to address burnout? The number one factor is to recognize it—to openly admit that it does exist and to advance a culture where it is OK for a physician to admit that they are experiencing burnout, talk about it, and ask for help. We have robust physician support services. We have a robust physician wellness program. We have a physician lead of physician wellness. All of these programs deal with physician burnout. We believe that openly attacking the issue and providing the physicians with tools is important.
The culture work is crucial. We need a culture of respect. We need to determine what a culture of professionalism looks like within a healthcare environment. We need to determine what teamwork looks like. When I was trained, we were not trained in teams, and the reality is that we now know that teams are an effective way of dealing with things including burnout.
HL: What are your primary clinical challenges now that the crisis phase of the pandemic has passed?
Finkler: We need to refocus on hospital-acquired infections such as central line–associated bloodstream infections and catheter-associated urinary tract infections. There are factors that have increased these infections during the pandemic such as new healthcare workers who do not understand the importance of the processes that were in place to keep these infections under control. As we enter a post-pandemic world, we are reteaching and restressing the importance of the processes that got us to low hospital-acquired infection rates.
Another area of focus is length of stay. We have watched our length of stay creep up. There are several reasons this has happened, and as we are pressured from both a workforce and capacity standpoint, we are going to have to put a heavy focus on length of stay. Within our institution, we have stood up a "mission control" that meets several times weekly to look at length of stay. There are lengths of stays that we will have trouble controlling—some of the outlier lengths of stays that may be due to unavailability of skilled nursing facility beds or long-term assisted care facility beds. You cannot solve those issues overnight.
There are things we can do to lower length of stay. We can expedite the discharge process. We can do what needs to be done during a hospitalization, then schedule other things that would be nice to have but not necessary to have as an outpatient service.
HL: What kind of workforce shortages are you experiencing at AdventHealth?
Finkler: We have workforce shortages not only in the nursing area but also in other disciplines, including pharmacy, radiology, laboratory technicians, and certified registered nurse anesthetists. It is important for everybody to recognize that the shortages do not stop in the nonphysician side—we are seeing physician shortages in several specialties.
HL: What are the primary efforts you have in place to address workforce shortages?
Finkler: The first thing we have done as an organization is taken a step back and said, "We understand that the pay must be competitive." In the pre-pandemic era, we would do market surveys every year or every other year. Now, we need to conduct market surveys more frequently. What was competitive a week ago may not be competitive four weeks from now. We are making sure that we are paying at the top of the market.
However, it is not just pay that is contributing to workforce shortages. It is also about benefits.
I am proud of our nursing innovation and workforce strategies that have helped stem the tide. We have gone from 3% turnover per month down to 1% per month. Things like working in a team model have helped.
We also are working on virtual nursing models. We recognize that we have a paucity of experienced nurses. Many of our nurses are young—many are graduate nurses. They do not have an enormous amount of experience, and they do not have a seasoned nurse to turn to on the floor. So, we have been working with experienced nurses in a virtual nurse model where they can cover several units in a hospital. They help the nurses on the floor with problems and questions, and they can do work such as discharges.
We have told our nurses if they want to go back to school to continue their education, we will pay for it, and they will be debt free. We also have been providing nurses more flexibility in scheduling. So, we are taking a proactive approach to the nursing shortage.
Inadequate access to mental health care is straining emergency departments, researcher says.
For pediatric patients with mental health conditions, prolonged lengths of stay in emergency departments increased significantly during the coronavirus pandemic, according to a new research article.
The pandemic has had a negative impact on the mental health of children due to factors such as caregiving disruptions and social isolation. Last month, the American College of Emergency Physicians and 34 other healthcare organizations raised alarm over the boarding of patients in emergency departments for days or weeks, including pediatric patients with mental health conditions.
The new study, which was published by the Journal of the American College of Emergency Physicians Open, is based on data collected from January 2020 to December 2021 at 107 emergency departments in 29 states. The study features several key data points:
At emergency departments, pediatric mental health visits with a length of stay greater than 12 hours accounted for 20.9% of all pediatric mental health visits
At emergency departments, pediatric mental health visits with a length of stay greater than 24 hours accounted for 7.3% of all pediatric mental health visits
At emergency departments, pediatric non-mental health visits with a length of stay greater than 12 hours accounted for 1.8% of all pediatric visits
At emergency departments, pediatric non-mental health visits with a length of stay greater than 24 hours accounted for 0.2% of all pediatric visits
The monthly counts of pediatric emergency department visits for mental health conditions peaked at 2,455 in September 2021
The monthly counts of pediatric mental health visits with a length of stay greater than 6 hours peaked at 975 in November 2021
At emergency departments, the most common diagnoses for pediatric mental health visits with a length of stay greater than 24 hours were suicide, self-injury, and depressive disorders
The data show aspects of the pandemic's negative impact on healthcare, the study's co-authors wrote. "In this sample of 107 EDs in 29 states, visit counts with prolonged LOS >24 hours more than doubled in some months since the arrival of COVID-19. These findings are indicative of an increasingly strained emergency and mental health system."
In a prepared statement, the lead author of the study said the data reflect a lack of access to mental health care in many communities.
"A cycle of compounding system failures is hindering care for many of our most vulnerable patients. Insufficient access to mental health care stands out among the factors that contribute to prolonged stays in the nation's emergency departments—there are too few options outside of emergency care for patients in many communities," said Alexander Janke, MD, MHS, national clinical scholar at the VA Ann Arbor Healthcare System and University of Michigan Institute for Healthcare Policy and Innovation.
The chief physician executive of Mercy says physician leaders need to know about the operational, strategic, service line, workforce, and financial aspects of healthcare.
Editor's note:This article appears in the March 2023 edition of HealthLeaders magazine.
Physician leaders should have fundamental knowledge of all aspects of healthcare, says the chief physician executive of the Mercy health system.
Jeffrey Ciaramita, MD, is senior vice president and chief physician executive at Mercy. A practicing cardiologist, he previously served in leadership roles at Mercy Clinic, a large medical group affiliated with Mercy.
Ciaramita recently talked with HealthLeaders about a range of issues, including physician leadership, workforce shortages, and patient safety. The following transcript of that conversation has been edited for brevity and clarity.
HealthLeaders: What are the main elements of physician leadership?
Jeffrey Ciaramita: Most people believe physician leadership is representing physicians. That would be a big mistake. Physician leadership is digging into the details and being a healthcare executive with fundamental knowledge of all foundational aspects of healthcare, including operational, strategic, service line, workforce dynamics, and financial.
Physician leadership is having a foundational understanding and using that foundation to inspire excellence in others, which includes other physicians and advanced practice providers. You need to inspire excellence, then lead change. Everyone inside and outside of healthcare knows that healthcare has evolved and changed over the years; and as we saw over the past couple of years, it will continue to change. The only way we are successful as physician leaders—whether it is a chief physician executive title or any other title—is if we can navigate and lead our teams through change.
HL: What is the status of physician burnout at Mercy?
Ciaramita: Luckily for us, Mercy partnered with the American Medical Association. We partnered with them to create a longitudinal study for physician burnout. As we were navigating the creation of this study and longitudinal surveys, COVID was just starting to hit.
Our initial AMA survey results showed us that we have a moderate amount of burnout in our ministry. It also showed us that we have a lesser degree of burnout within Mercy than the national averages. That being said, overall for physicians and staff if we look at burnout, there is no question it has probably been at one of the higher levels throughout most people's careers.
We have gone through our second round in the longitudinal study and are awaiting those results. My suspicion based on early indicators is that we are improving. There is a feeling among our staff that there is a light at the end of the tunnel.
HL: What are the primary initiatives you have in place to address physician burnout?
Ciaramita: We have a Rapha program that has an app associated with it. Rapha comes from the Hebrew word "to heal." That is a confidential program, where physicians can mentor and be resources to other physicians who have self-identified themselves as struggling. They want to connect and discuss issues. We have had this program in place for a few years.
Last year, Mercy adopted universal usage of Schwartz Rounds. Schwartz Rounds are co-worker events that are in a grand rounds type of style. They either focus on a medical case or a theme related to the emotional impact of patient care. Staff members talk about a case or talk about the theme, and they can navigate their own experiences and feelings with a sense of community. Schwartz Rounds can be 10 people or 100 people.
We have Mercy Mission Teams, which have paired up with new physician wellness leaders to have wellness, mission, and culture committees.
This all is in addition to our employee assistance program, which allows 24/7 access for any employee to professional resources.
Jeffrey Ciaramita, MD, is senior vice president and chief physician executive at the Mercy health system. Photo courtesy of Mercy.
HL: What are your primary clinical challenges now that the crisis phase of the coronavirus pandemic has passed?
Ciaramita: The big one is providing the breadth and the quality of clinical care with the highest level of patient satisfaction in the setting of a massive workforce challenge. Finding enough staffing and retaining enough staffing throughout our clinical areas is a challenge.
HL: What kind of workforce shortages are you experiencing at Mercy?
Ciaramita: Our workforce shortages are similar to the trends nationally. Within Mercy, our biggest challenges are in the areas of support services and clinical services. We have shortages in nurses, medical assistants, medical receptionists, imaging technicians, operating room technicians, and other positions.
Most of the shortages are not simply because of wages. Most of the shortages are the result of a workforce that demands flexibility … such as changes to their work schedule.
From our perspective, our number one strategy for workforce shortages is focused on retention. We have many great employees, which are the singular reason for why we are a high-quality ministry, and we have achieved some of the best patient satisfaction in the country. We know that comes from the employees who are with us today.
HL: What are you doing in terms of recruitment and retention?
Ciaramita: We have refined our recruitment process. We have identified areas to improve the onboarding of every employee who works within our ministry. We have shortened the timeline when someone applies for a job. We have made a lot of our recruitment electronic and user-friendly.
We have offered several different types of bonuses such as sign-on bonuses and bonuses for referral of new employees. We are keeping up with the market, and we are making sure that we are valuing employees financially with compensation that is commensurate with our desire to bring in the best of the best. We are also partnering with educational institutions to help build a pipeline of future employees.
We are continuing to refine our work toward automation. This is not automation to eliminate positions. It is automation to augment positions—knowing that as healthcare demands grow as our communities age and the demand for complex care grows, we will likely never have enough human beings to deliver care. We will continue to work on automating tasks, while we are partnering with institutions to build a pipeline of nurses, advanced practice practitioners, medical assistants, operating room technicians, and other healthcare workers.
I cannot stress enough the financial, cultural, quality, and distinct workforce benefits by focusing on retention. We hold town halls—we are assessing how we can meet the needs of our staff.
We have created a gig workforce program. Our gig program is similar to agency or contracted labor. We created our own internal program that provides flexible hours and ease of scheduling. So, for our own nurses, for example, some of whom may work 40 hours a week or some of whom may work 30 hours a week, they can go into our gig program and pick up an additional two hours, or four hours, or 16 hours if they want. They can work in different areas, but they are still Mercy employees. They can work when they want, how they want, and in the setting that they want.
HL: What are the primary elements of patient safety at Mercy?
Ciaramita: We have instilled in our co-workers—our clinicians and every single person who has the honor to touch a patient that we serve—a culture of first and foremost do no harm. If you look at Mercy's commitment to quality, we have made a commitment in every community that we serve to be the number one high-quality healthcare provider by nationally reported metrics.
We have created a culture of reporting that not only covers lapses in care and errors but also promotes reporting of near misses. In near misses, there was not a safety event but there could have been a safety event. Our co-workers are focused on learning from errors and near misses rather than having a punitive approach. How can we find out what happened? How can we document an incident? How can we bring in a team to do an analysis to make sure that we can broaden our educational opportunities about what happened in every community we serve? This work is reflected in our high quality scores.
We utilize our electronic health record to create alerts to avoid medication errors and vaccine administration errors. We have very robust systems in our EHR to avoid those errors.
I would put our patient safety under the auspices of our dedication to an overall high-quality system. That high-quality system within our ministry all falls under a newly created department called the Office of Clinical Excellence. This department is using evidence-based medicine, technology augmentation, and a humanistic approach to education, culture, and learning to drive patient safety.
A new institute at the health system will focus on kindness research, fostering healthier communities, workforce development, and health justice.
CommonSpirit Health has launched the Lloyd H. Dean Institute for Humankindness & Health Justice.
Research has shown that kindness in clinical care can decrease patients' stress and emotional turmoil. The new institute is designed to use the power of kindness to treat the social causes of poor health and advance health justice.
The institute is named after Lloyd Dean, former CEO of CommonSpirit.
Evidence shows that kindness, compassion, empathy, and trust in clinical care impact healthcare outcomes, says Alisahah Jackson, MD, president of the institute.
"We have decades of research about kindness, compassion, empathy, and trust. There are multiple organizations that have been doing this research. CommonSpirit partnered with Stanford several years ago to look at how kindness, compassion, and altruism in a healthcare setting can influence health outcomes. There were a couple of things that were discovered. We found that patients who received compassionate care from their providers were better adherent to their medication regimens. We found that patients who went into surgery and received compassionate and kind care afterwards healed faster," she says.
Kindness is particularly powerful, Jackson says. "We know that kindness can lower anxiety levels. Research has shown that kindness can lower blood pressure. So, there is research that tells use there are tangible outcomes for individuals when they receive kindness and when they give kindness. There is research that shows people have better mental health outcomes when they are participating in random acts of kindness or volunteering for the common good."
The institute has four focal points, she says:
"One is humankindness in action. That will be looking at how we accelerate the research that has already been done in clinical settings. We also want to bring new research forward."
"The second area will continue our organization's focus on healthier communities. We all now recognize the terms social determinants of health or social drivers of health as well as the impact they have on all of us in terms of health outcomes. At CommonSpirit, social determinants of health have long been a component of our mission to build healthier communities."
"The third area is focused on workforce development and pipeline programs. If we are going to be honest about addressing justice in this country, we must make sure we are addressing economic mobility and financial stability. This is important for CommonSpirit because we tend to be anchor institutions in the communities that we serve. One of our goals is to think about pipeline programs earlier. Many times, pipeline programs start in high schools. But we know that girls in particular start losing interest in science, technology, engineering, and math in middle school. We need to see whether there are things we could be doing to keep their interest in STEM fields sooner—even in elementary school."
"The fourth key area is the notion of health justice. This will require a lot of strategy around policies. I like to think of it as 'Big P' policies and 'little p' policies. Big P policies include federal, state, and local government policies. The little p policies are organizational policies—sometimes we have policies in place at healthcare organizations that unintentionally drive disparities. We need to be constantly reviewing policies with a social justice and health equity lens."
Institute as accelerator
The institute is going to build on work that is ongoing at CommonSpirit, Jackson says. "The institute is going to serve as an amplifier and accelerator of great work that is already happening. We are already connecting community resources to clinical care. One of the things that our community health division runs is a program called the Connected Community Network, which is a program that allows for patients to be connected to community resources because they are screened for social needs in our clinical care settings."
The Connected Community Network program is a powerful tool for clinicians, she says.
"As a family medicine provider that means I can screen my patients for social determinants of health. If they screen positive, where there is a Connected Community Network, I can make a referral for my patients to community organizations to have needs addressed. Ultimately, our goal is once those needs are addressed and I can have a conversation with the patient to make sure they are getting the things that they need, by getting those social needs addressed that starts to help them in their healthcare outcomes. Those are the types of programs that the institute will be looking to accelerate across our entire organization."
In some specialties such as nutrition and genetics, telehealth visits can often replace in-person visits, researchers found.
In a new study that looked at more than 30 specialties, most patients who had a specialty telehealth visit did not require an in-person follow-up visit in that specialty over the next 90 days.
Since the beginning of the coronavirus pandemic, telehealth visits have increased dramatically. The millions of telehealth visits that have been conducted since the beginning of the pandemic are an opportunity for researchers to assess the utilization of telemedicine.
The new study, which was conducted by Epic Research, examined more than 35 million telehealth visits conducted between March 1, 2020, and May 31, 2022. The research includes several key findings:
The two specialties that showed the fewest in-person follow-up visits in the 90 days after a telehealth visit were genetics (4% of telehealth visits) and nutrition (10% of telehealth visits)
In specialties that often involve consultations such as genetics and nutrition, telehealth visits could replace the need for in-person visits
The two specialties that showed the most in-person follow-up visits in the 90 days after a telehealth visit were obstetrics (92% of telehealth visits) and fertility (54% of telehealth visits)
For specialties that showed relatively high numbers of in-person follow-up visits, the in-person visits were likely related to needing additional care rather than duplicative care
Mental health and psychiatry had the highest volume of telehealth utilization as well as one of the lowest numbers of in-person follow-up visits in the 90 days after a telehealth visit (15% of telehealth visits)
"These findings suggest that, for many specialties, telehealth visits are typically an efficient use of resources and are unlikely to require in-person follow-up care. If telehealth is not duplicative of in-person visits for those specialties, it can be an effective tool to help expand access to care," the study's co-authors wrote.
Interpreting the data
The lead author of the study, Jackie Gerhardt, MD, vice president of clinical informatics at Epic, told HealthLeaders that the relatively low numbers of in-person follow-up visits after a telehealth visit is significant.
"We specifically organized the study to look at what happened in the three months following a telehealth visit to find out whether or not someone needed an in-person visit within that three months. Our reasoning was that if you need a follow-up visit in that three months, it was likely that the visit was for the same condition. For example, you might have an orthopedic telehealth visit to talk about hip pain, and if you got the right recommendations that you needed, you probably would not need a follow-up visit in-person within orthopedics. So, we concluded that in specialties that did not need follow-up in-person, it was likely that the telehealth visit was able to stand on its own."
Nutrition and genetics are examples of where telehealth visits could replace in-person visits, she said. "If you are asking for advice on nutrition or reviewing your genetic history, both of those can be transactional such that you get information that you need from a single consult, and it does not necessarily require a physical exam. The ability to do that during a telemedicine visit is very similar to information you would be gathering in-person. So, it could increase access and potentially improve the way that people can get care because they do not have to travel to a clinic and can more readily access their provider."
Telehealth visits are an effective tool to help expand access to care, Gerhardt said. "Telehealth visits are part of our general advancement in healthcare toward being consumer-centric and patient-centric. Different organizations structure telemedicine in different ways; but in some cases, instead of having to stick to the 8-to-5, Monday-through-Friday services of in-person care, you can get more access in terms of the number of days and time slots through telehealth as well as get a visit more quickly than you can get an in-person visit."
The study shows that telehealth visits can supplement or replace many in-person visits, she said. "Telehealth visits will never replace all in-person visits; but for specific specialties and specific types of visits, telehealth can serve as an adjunct or a replacement."
The study's computer model included age-stratified demographics, risk factors, and immunological dynamics of infection and vaccination.
U.S. COVID-19 vaccinations have averted more than 18.5 million additional hospitalizations and about 3.2 million additional deaths, according to a new study.
The coronavirus pandemic is among the deadliest outbreaks in U.S. history, killing more Americans than those lost in the 1918 influenza pandemic. Vaccinations for COVID-19 in the United States started two years ago, and more than 655 million doses have been administered, according to the new study.
The new study, which was conducted by The Commonwealth Fund, is based on a computer model for data from December 2020 to November 2022 that included age-stratified demographics, risk factors, and immunological dynamics of infection and vaccination. The research features four key findings:
COVID-19 vaccinations averted more than 18.5 million additional hospitalizations
COVID-19 vaccinations averted about 3.2 million additional deaths
COVID-19 vaccinations averted nearly 120 million additional infections
COVID-19 vaccinations averted about $1.15 trillion in medical costs
COVID-19 vaccinations have been effective with multiple benefits, the study's co-authors wrote. "The unprecedented pace at which vaccines were developed and deployed has saved many lives and allowed for safer easing of COVID-19 restrictions and reopening of businesses, schools, and other activities. This extraordinary achievement has been possible only through sustained funding and effective policymaking that ensured vaccines were available to all Americans. Moving forward, accelerating uptake of the new booster will be fundamental to averting future hospitalizations and deaths."
The reduction in COVID-19 infections is a crucial accomplishment, the co-authors wrote. "Vaccination also has prevented many millions of COVID infections. Although the acute phase of these infections may not have required medical attention, each infection carries a risk of long COVID and debilitating symptoms. Many of the prevented infections would have been reinfections, which have higher risk of death compared to initial infections."
The averted infections, hospitalizations, and deaths are significant, they wrote. "Without vaccination the U.S. would have experienced 1.5 times more infections, 3.8 times more hospitalizations, and 4.1 times more deaths. These losses would have been accompanied by more than $1 trillion in additional medical costs that were averted because of fewer infections, hospitalizations, and deaths."



 Marc Napp, MD, MS, executive vice president and chief medical officer of Memorial Healthcare System. Photo courtesy of Memorial Healthcare System.
Marc Napp, MD, MS, executive vice president and chief medical officer of Memorial Healthcare System. Photo courtesy of Memorial Healthcare System.




 Jeffrey Ciaramita, MD, is senior vice president and chief physician executive at the Mercy health system. Photo courtesy of Mercy.
Jeffrey Ciaramita, MD, is senior vice president and chief physician executive at the Mercy health system. Photo courtesy of Mercy.

_0.jpg?itok=PTnLLP2z)