Almost 80% of physicians surveyed by the AMA say patients are skipping care because of delays in prior authorizations.
Prior authorizations are a consistent pain point in revenue cycle operations, and a new survey shows just how detrimental they are for patients.
According to the American Medical Association’s annual prior authorization survey, 78% of physicians said issues with prior authorization resulted in patients forgoing care.
The survey of 1,000 practicing physicians offers some significant insights to the negative impact of prior authorization on the patient’s care experience:
94% said prior authorization “always, often or sometimes” delayed a patient’s access to necessary care.
19% said prior authorization resulted in an event leading to a patient being hospitalized.
13% said prior authorization resulted in an event leading to a life-threatening event or requiring intervention to prevent permanent damage.
7% said prior authorization resulted in an event leading to a patient’s disability, permanent bodily damage, congenital anomaly, birth defect or death.
Prior authorizations are a significant problem for providers as well, with many having to rely on multiple staff to work on them, according to a 2023 survey by the Medical Group Management Association.
Another report by the Kaiser Family Foundation found that 6% of the 35 million prior authorization requests submitted to Medicare Advantage in 2021 were denied. Of those denials, only 11% were appealed, and of that group, 82% were fully or partially overturned.
Some health systems, like University Health KC, have turned to tech solutions to manage prior authorizations, and seen some results.
“Within about two months of kicking off implementation, [the program] started going to payer websites and logging requests for prior authorizations by taking that information out of our EMR,” Seth Katz, vice president of revenue cycle and HIM, previously told HealthLeaders.
In January, the Centers for Medicare and Medicaid Services finalized the Interoperability and Prior Authorization Rule, setting requirements to streamline the process for Medicare Advantage, the Children’s Health Insurance Plan (CHIP), and Medicaid managed care plans, among others.
The rule adds provisions to increase data sharing, in turn, reducing the administrative burden on providers, enabling them to spend more time providing care. For example, as part of one requirement for the rule, payers must send prior authorization decisions for expedited requests within 72 hours. For standard requests, decisions must be sent within seven calendar days.
The rule is expected to result in $15 billion in savings over the next 10 years.
The proposed 2025 Medicare Physician Fee Schedule puts more financial pressure on providers.
The proposed 2025 Medicare Physician Fee Schedule puts more pressure on providers’ billing practices as well as their bottom line.
The Centers for Medicare and Medicaid Services (CMS) is poised to cut physician reimbursement by 2.8%, making it the fifth consecutive year of payment cuts. This, along with the anticipated 3.6% increase to practice costs due to inflation, does not bode well for revenues.
“The cost of healthcare is rising. There is clearly inflation in our economy, and having the reimbursement go down is absolutely the wrong direction,” Andy Anderson, executive vice president and chief medical and quality officer at RWJBarnabas Health, previously told HealthLeaders.
“The Physician Fee Schedule model is not sustainable if the reimbursement is going to be cut,” he added.
According to Anderson, the reimbursement needs to keep pace with inflation and healthcare costs.
The proposed rule will also tackle suspicious billing practices in Medicare’s Shared Savings Program, taking improper payments into account when revisiting the shared savings and shared losses calculations for accountable care organizations. Earlier this month, CMS proposed a rule examining the program’s billing activity after noting a significant increase in “highly suspect” claims.
In addition to the reimbursement cut and increase billing scrutiny, a health equity benchmark, similar to that used for the ACO REACH Model, would be adopted to incentivize organizations in more rural and underserved areas to participate.
CMS will accept public comments on the proposed 2025 PFS until September 9.
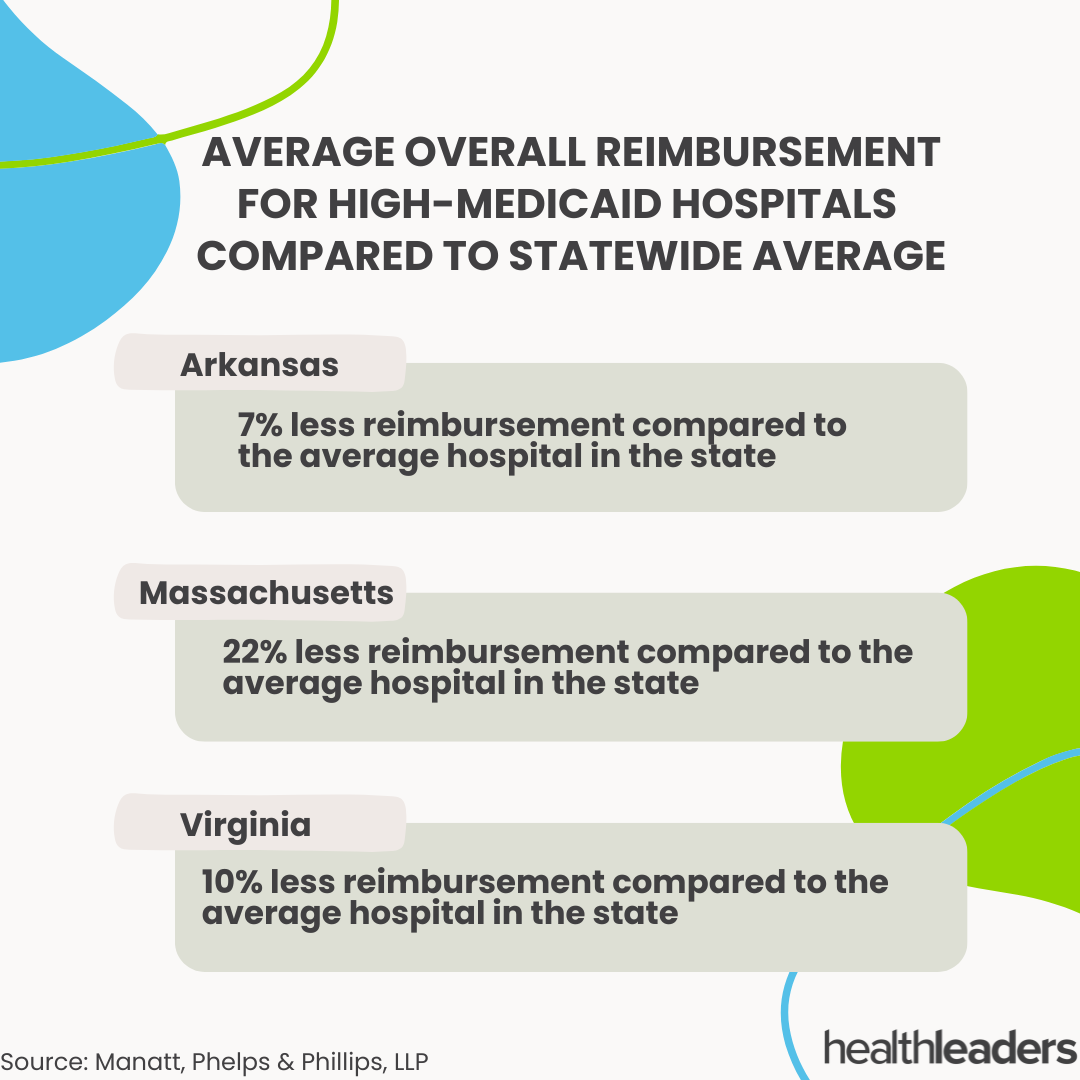
A new report by Manatt Health found that high-Medicaid hospitals were reimbursed up to 22% less than average hospitals.
Examining hospital data from Arkansas, Massachusetts, and Virgina, the report found that high-Medicaid hospitals received less overall reimbursement compared to the average hospitals within their respective states. The data of the report reaffirms previous studies claiming high-Medicaid hosptials are at a financial disadvantage when it comes to reimbursement.
Here are four HealthLeaders articles that emphasize the importance of efficient, and compliant, billing practices.
As the healthcare sector becomes more consumer focused, providers must make sure their billing practices are up to standard and patient friendly. Patients are responsible for paying more of their healthcare costs, there’s also the need to adopt different methods of payment to ensure cash flow.
Simon C. Mathews, MD and Martin A. Makary, MD, both professors at Johns Hopkins University, proposed five metrics providers can use to measure billing quality. These metrics include whether or not the provider offers itemized bills, provides pricing information to patients when asked, or if patients are able to speak with billing representatives about their bill.
“In the same way medical complication rates are collected for improvement purposes, and some are available to the public,” an article on the professors stated, “Metrics of billing quality could be used to create public accountability for US hospitals.”
There’s very little room for error when it comes to billing, and providers must be meticulous to ensure patients and insurers aren’t over or under paying for the care they receive. This article offers insights from HealthLeaders’ 2023 RevTech Exchange, one revenue cycle executive who suggests forming a team to oversee price transparency efforts, and how patient portal utilization can help with collections.
A study from the University of Southern California eased some concerns from federal agencies about predatory billing practices. Of a random sample of hospitals, one in 10 hospitals were found to employ predatory billing practices like interest-bearing payment plans.
Of all the providers surveyed, 87% offered interest-free payment plans.
In 2022, UAB Selma Family Medicine Center decided to adopt a new practice management system to improve billing inefficiencies. The center was struggling financially and administrative director Jeff Denney, saw the potential to for technology to help stabilize things.
With the implementation of the new practice management system, Selma Family Medicine saw a reduction in overall denials and days in accounts receivable, and an increase in their gross collection rate.
One health system has already filed a lawsuit, could it happen to you?
The Supreme Court’s reversal of the so-called Chevron case could impact many healthcare organizations’ revenue cycle operations.
Under the initial ruling made in 1984, judges would defer regulatory disputes to federal agency interpretations of a law. With the Supreme Court voting 6-3 to roll back this decision, the healthcare sector may see a wave of litigation around reimbursement and insurance eligibility.
On June 3, the same day the Chevron deference was overturned, Hackensack Meridian Health filed a lawsuit against the Centers for Medicare and Medicaid Services (CMS). The New Jersey-based health system claims the low reimbursement rates for Medicaid Disproportionate Share Hospital payments have cost three of its hospitals—University Medical Center, Jersey Shore University Medical Center, and Raritan Bay Medical Center—almost $600,000.
In a statement on the system’s website, health system leaders claim that CMS “deprived hospitals of some of reimbursements they are due and the data to check their reimbursement rates.”
“The lawsuit also challenges CMS’ refusal to enable hospitals to effectively employ the congressionally mandated procedures for obtaining relief from these underpayments,” the statement said.
In addition to increasing its DSH payments, as part of the lawsuit, the system wants the interpretation of a low-income patient to be broadened.
Hackensack Meridian Health’s lawsuit could be the first of many to challenge CMS’ reimbursement rules. With more flexibility around the interpretation of a law, providers have some leverage when beginning legal proceedings.
However, the odds aren’t entirely in their favor. Judges may opt to ignore federal agency interpretations of laws in favor of exercising independent judgement, which could mean inconsistent rulings for similar cases.
The overturning of the Chevron deference may make it harder for HHS’ future efforts—which could have a negative effect on public health. Proposed rules for minimum staffing requirements in nursing homes and the development of new programs are now prone to being challenged.
There's a rev tech solution for just about every revenue cycle process and even more vendors.
MaryAnn Murphy (Assistant Vice President of Revenue Cycle, Northwell Health) shares why her system prefers to use multiple vendors and Shawn McCardell (Associate Vice President of Revenue Cycle, Frederick Health) shares why his system opts to have all solutions come from one vendor.
Payers and difficulties with eligibility and prior authorizations keep patients from getting the care they need.
Seth Jeremy Katz (VP Revenue Cycle and HIM, University Health KC) discusses the difficult, and often frustrating, process of working with payers on eligibility and prior authorization claims.
Hospitals must add a footer at the bottom of their homepage with a link to the report.
Hospitals are now required to report price information in a “standard machine-readable” format, with data specification and a data dictionary.
The requirement is part of a price transparency rule enacted this week by the Centers for Medicare & Medicaid Services (CMS).
The new format, designed to make it easier for patients to understand hospital charges, is part of the 2024 Hospital Outpatient Prospective Payment System and ASC rule. Additionally, the rule mandates that hospitals add a footer at the bottom of their homepage with a link to the file, as well as including a .txt file in the website’s root folder.
Hospitals found to be out of compliance will receive a warning and be required to submit an acknowledgement of receipt.
As patients shoulder more of the cost for their healthcare, providers are feeling more pressure to ensure price transparency and abide by the No Surprises Act.
In February, CMS data showed that the number of surprise billing disputes had risen each quarter since the legislation went into effect. The majority of disputes, the agency found, came from a small group of providers.
Providers affected by the Change ransomware attack were tossed a lifeline and CMS tackles suspicious billing.
As the dust from a hectic first half of the year begins to settle, organizations are aiming for a strong finish. However, there are a few loose ends that need to be addressed.
Here are some revenue cycle news stories you may have missed.
Months after the Change Healthcare ransomware which disrupted the operations of providers across the country, many are still struggling to rebound. Some providers have been unable to begin the independent resolution process for out of network claims, being unable to access the information they need to proceed with billing.
The Biden administration, under the No Surprises Act, is giving providers until October 12 to begin the negotiation process for services provided this year, with the possibility of the deadline being extended.
To ensure patients and their care team have access to their health information, the Health and Human Services Department finalized a rule establishing penalties for health systems that prevent them from doing so. Various disincentives were also established to further dissuade providers from blocking patient’s access to information.
The rule, initially proposed in 2023, is backed by the 21st Century Cares Act.
The Centers for Medicare and Medicaid Services (CMS) proposed a new rule to address suspicious billing activity within the Shared Savings Program. The rule excludes payouts for codes relating to significant, anomalous, and highly suspect (SAHS) claims from being used to assess the financial performance of accountable care organizations.
The rule is part of larger plan to address anomalous spending in the program.
After noting a significant increase in highly suspect claims for Healthcare Common Procedure Codes (HCPCS), The Centers for Medicare & Medicaid Services (CMS) is proposing a new rule to crack down suspicious billing activity.
CMS officials have reported a significant increase in SAHS (significant, anomalous and highly suspect) claims for codes for urinary catheters, tips, and insertion supplies during 2023, and the corresponding HCPCS codes were flagged for SAHS billing.
The proposed rule will exclude payouts for codes A4352 and A4353 on DMEPOS claims from the expenditure and revenue calculations used to assess financial performance for accountable care organizations (ACO) for 2023. These calculations will also establish benchmarks for organizations starting agreements in 2024, 2025, and 2026.
The decision comes as part of a larger strategy to address SAHS claims within the Medicare Shared Savings Program, which will be explained further in the CY 2025 Physician Fee Schedule.
In a statement, Jennifer Holloman, the American Hospital Association’s senior associate director of policy, said the rule is a “significant” step to address anomalous spending, and it won’t be the last.
“We hope the upcoming CY 2025 Physician Fee Schedule will provide additional details to support longer term strategies to address anomalous spending,” she said.
According to CMS, the proposed rule could delay the disbursement of initial ACO payments for 2023 by up to six weeks.





.jpg?itok=kyzbHb-K)

.png?itok=y45eD41N)


