The CFO of Montage Health detailed three financial priorities for his hospital.
CFOs need to remain vigilant in their financial planning, and Matt Morgan, MBA, FACHE, FHFMA, CFO of Montage Health’s Community Hospital, will be doing this by prioritizing three key items for his hospital.
From growing responsibly to evaluating capacity, one CFO has a few financial priorities for his hospital this year.
The median calendar year-to-date operating margin index for hospitals is reflecting an ongoing improvement, however, leaders are not off the hook.
CFOs need to remain vigilant in their financial planning, and Matt Morgan, MBA, FACHE, FHFMA, CFO of Montage Health’s Community Hospital, will be doing this by growing responsibly, evaluating capacity, and focusing on performance improvement.
How will Morgan get this done? Read on to find out.
Community Hospital is part of Montage Health—a locally owned, nonprofit network of healthcare providers with more than 250 hospital beds and 28 skilled nursing beds located in Monterey County, California.
The hospital is currently growing certain service lines to better serve its community and region, Morgan says.
So, supporting that clinical growth with key decisions on infrastructure, funding, staffing, and performance monitoring will be critical to its financial success.
On top of growing responsibly, Community Hospital also plans to evaluate its capacity.
“The hospital’s occupancy rates continue to climb, and forward projections suggest continued pressure on existing capacity,” Morgan says. “As CFO, active participation in evaluating service needs, structural design, patient throughput and capital forecasts are significant efforts in 2024.”
Performance improvement is also top of mind for Morgan.
“While volume and revenue growth has been excellent these past five years, forward projections suggest that cost growth may exceed revenue growth,” he says.
This means that continued detailed evaluation of performance improvement at the hospital, medical group, urgent care, and insurance settings is paramount Morgan says.
“Past financial success is not always indicative of future results!”
CFOs meticulously sift through quarterly earnings reports, but what do the results from some of the biggest in the nation tell us about the overall trends?
Now that health system financial results for the third quarter and first nine months of 2023 have all come in, it gives CFOs a chance to examine the overall trends.
With many making improvements on the back of some challenging financial years, operating losses, high expenses, and labors costs still weighed heavy on some of the biggest health systems in the nation—meaning these issues were surely exacerbated for smaller hospitals.
Several healthcare systems, such as CommonSpirit and Community Health Systems, reported increased operating losses compared to the previous year. This trend indicates continued financial challenges and the need for cost management strategies.
Revenue growth.
Despite the challenging financial environment, many healthcare systems, including Trinity Health, Christus Health, and HCA Healthcare, reported an increase in operating revenue. This suggests that there is potential for generating more income, although it is crucial to control expenses to improve overall profitability.
Higher expenses.
Most healthcare systems experienced an increase in expenses, particularly in terms of employee compensation and benefits, as well as supply costs. Hospital CFOs should closely monitor expense growth and implement strategies to manage costs effectively.
Net income fluctuations.
Net income varied among the healthcare systems analyzed. While some, like Kaiser Permanente and Universal Health Services, reported an increase in net income, others, such as Renton-based Providence, experienced larger operating losses. CFOs should focus on optimizing revenue streams and managing expenses to drive positive net income.
Impact of investments.
CommonSpirit and Providence reported significant net investment losses, impacting their overall financial performance. CFOs should carefully evaluate investment strategies and their potential impact on the organization's financial health.
Operating margin changes.
Tenet Healthcare reported a decrease in operating income, resulting in a decline in the operating margin. Hospital CFOs should monitor and analyze their organization's operating margin to ensure financial stability and sustainability.
Positive financial performance.
Despite the overall challenging environment, some healthcare systems, including Christus Health and Mayo Clinic, reported improved operating income and net income. CFOs should study the strategies employed by these organizations to identify potential best practices.
Providence and Mayo Clinic reported higher expenses due to wage increases. Hospital CFOs should pay special attention to labor costs and develop strategies to manage these expenses effectively.
As for the future? Not much is changing in terms of strategy. Hospital and health system CFOs need to continue to focus on optimizing revenue, controlling expenses, monitoring investments, and implementing cost management strategies to navigate the complex financial landscape.
While this news shouldn’t shock CFOs, longer-range capital plans and strategic investments will still need to be of focus. In fact, S&P says that additional spending or debt issuances could be a factor influencing credit quality, depending on balance-sheet strength and the level of cash flow improvement.
Here are nine takeaways from the report that hospital and health system CFOs should take into consideration this year.
Labor expenses remain a major challenge:
Ongoing cash flow margin pressures are primarily due to labor expenses.
The slow easing of labor expense pressures is complicated by factors such as union activity, regional market difficulties, higher base labor rates, and challenges in international recruitment.
CFOs should focus on accelerating revenue growth, improving staffing efficiencies, and making non-labor expense reductions to enhance earnings and cash flow.
Potential impact on credit ratings:
The negative sector view is influenced by the strain on cash flow, with labor and other inflationary expenses contributing to ongoing challenges.
Credit rating performance will depend on revenue trends and management's ability to achieve offsetting efficiencies.
CFOs need to closely monitor credit quality trends, with a particular emphasis on the pace of margin recovery and the ability to improve operating performance.
Balance sheet considerations:
While balance sheets remain sound, they have not strengthened materially for most organizations.
CFOs may face reduced balance-sheet flexibility as they consider capital needs and spending strategies, especially if they restart deferred capital projects or utilize debt.
Strategic spending should be carefully managed to avoid additional pressure on the balance sheet and increased carrying costs.
Varying credit quality trends:
There is a higher percentage of negative outlooks across credit ratings, with ongoing uncertainties in credit stability.
Organizations in demographically favorable regions, with healthy demand, market positions, and favorable payer rates, are more likely to perform in line with rating expectations.
Cash flow recovery in 2024 will be a crucial factor influencing credit quality assessments.
Challenges for lower-rated entities:
Lower-rated entities may face a difficult 2024 without meaningful partnerships or improved labor conditions.
Sustained higher interest rates, tighter lending, and limited debt capacity could impact capital spending for lower-rated organizations.
CFOs of lower-rated entities should seek strategies to address ongoing covenant issues and strengthen their financial positions.
Industry-specific challenges:
Revenue is strained by payer and service mix dynamics, with challenges in governmental payments, Medicaid, and commercial payer rates.
CFOs should navigate the shift from inpatient to outpatient services, manage commercial payer relationships, and address difficulties in claims processing and denial rates.
Efficiency focus and operating model improvement:
Management teams are accelerating expense management initiatives to lower the cost base.
Outsourcing to third parties, increased use of AI, asset sales, service line consolidation, and reduction in operating leases are strategies to improve efficiency.
CFOs should assess these initiatives based on cash flow, growth potential, and diversification of the revenue base.
Capital spending and debt issuance challenges:
Debt issuances have slowed, but CFOs must balance the need for capital spending with rising interest rates and weaker operating performance.
Access to capital may be difficult for lower-rated entities, potentially putting them at a long-term strategic disadvantage.
CFOs should consider less cash-intensive strategies and carefully manage debt-like structures, such as operating leases.
Event risks and ongoing pressures:
Cybersecurity events, weather, and other physical risks pose ongoing pressures on organizations.
CFOs should allocate resources for planning and investment to minimize financial and operating disruption from unexpected events.
Event risks could impact financial and management resources, affecting performance improvement needed to maintain credit ratings.
There are six major challenges that are forcing CFOs to pull the plug on payer contracts.
The payer/provider battle is raging, and signaling what may be an emerging trend: More organizations are fighting back against payers by terminating their contracts completely.
What exactly has led to the turmoil? CFOs say the reasons are vast, but below are six reoccurring challenges shared to HealthLeaders by hospital and health system CFOs and CEOs.
The great termination? More organizations are terminating payer contracts amid heated negotiations, and Medicare Advantage is in the hot seat.
The payer/provider battle is raging, and signaling what may be an emerging trend: More organizations are fighting back against payers by terminating their contracts completely, and Medicare Advantage (MA) has seemingly been the focus.
Thanks to record inflation and operational challenges, hospital and health systems find themselves with their backs against the wall in negotiations, leading CFOs to initiate contract terminations.
But what exactly has led to the turmoil? CFOs say the reasons are vast.
“Bad behavior.”
More organizations are now considering contract terminations due to dissatisfaction with reimbursement rates and overall bad payer behavior.
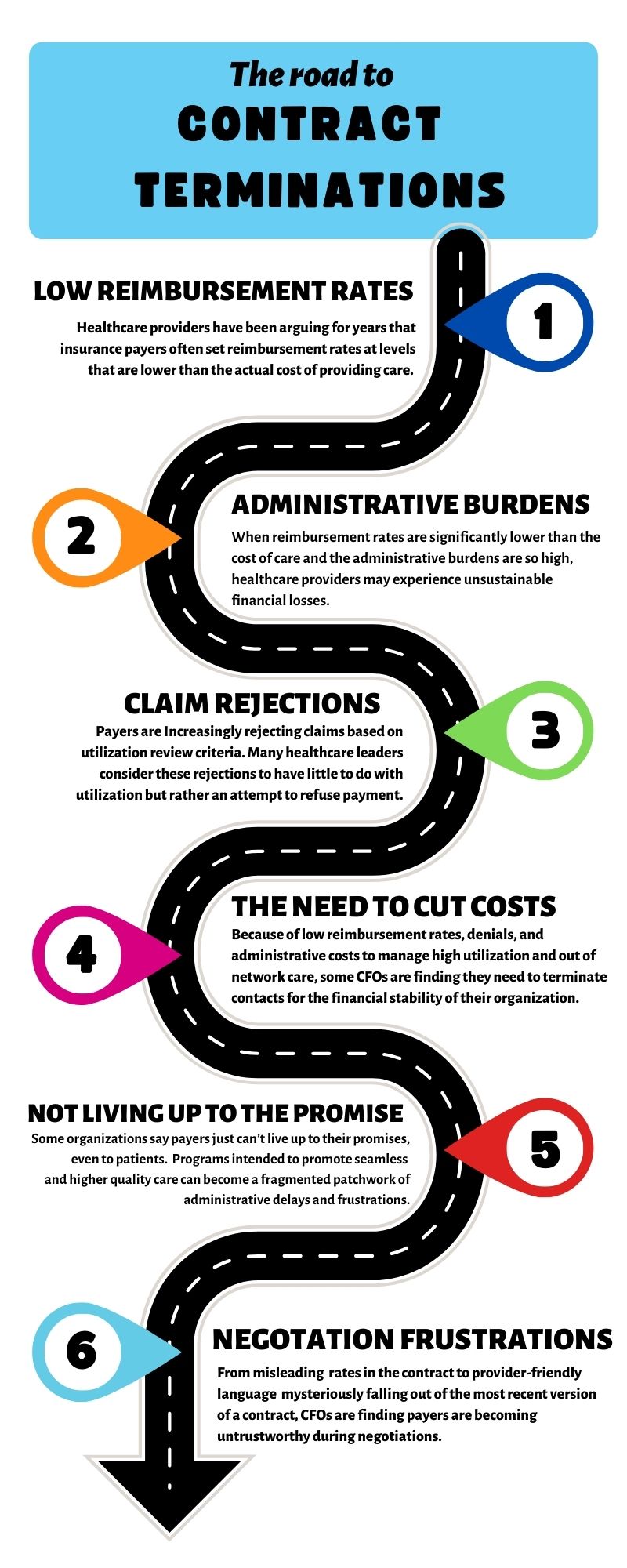
Healthcare providers have been arguing for years that insurance payers often set reimbursement rates at levels that are lower than the actual cost of providing care. Couple this with skyrocketing inflation costs and labor expenses, and providers can be left with no other choice.
When reimbursement rates are significantly lower than the cost of care and the administrative burdens are so high, healthcare providers may experience unsustainable financial losses. These underpayments along with egregious denials are pushing providers to the limit.
In such cases, CFOs may weigh the option of contract termination as a last resort to protect the financial stability of the organization.
“There is rarely one final straw, but rather, a cumulation of events that negatively impact the fiscal viability of the relationship,” Britt Berrett, managing director and teaching professor at Brigham Young University and former CEO with HCA, Texas Health Resources, and SHARP Healthcare, explained.
“Long before rates become contentious, hospitals are dealing with bad behavior and payer shenanigans,” Berrett said.
For example, he says, payers are rejecting claims based on utilization review criteria. Many healthcare leaders consider these rejections to have little to do with utilization but rather an attempt to refuse payment.
Luckily for providers, organizations are becoming more capable of cost accounting and utilizing analytics to determine the actual cost by patient and payer.
Why Medicare Advantage?
Why has MA been in the hot seat of terminations? While not the only culprit of the turmoil, organizations have been fighting back against MA’s low reimbursement rates for years, and as Berrett said, maybe CFOs are finding no fiscal viability in the relationship with the payer.
One case in point is Scripps Health. Two medical groups within the system canceled their MA contracts for 2024 because of low reimbursement rates, denials, and administrative costs to manage high utilization and out of network care.
“We’re unfortunately on the vanguard of what I think is going to be a very ugly few years between hospitals and commercial insurance companies,” Chris Van Gorder, president and CEO of Scripps, told USA Today.
And Scripps has the resources to better manage these burdens, meaning these burdens are even more exacerbated for smaller systems.
An example of this is Samaritan Health Services. It recently terminated its commercial and MA contracts with UnitedHealthcare.
The five-hospital, nonprofit health system cited slow processing of requests and claims that have made it difficult to provide appropriate care to UnitedHealth's members, according to a news release from Samaritan.
“This, along with other factors, is not in alignment with our mission of building healthier communities together,” the health system said.
Another example is St. Charles Health System, a four-hospital network and healthcare company in Central Oregon, which terminated its MA contracts in 2023.
Steve Gordon, president and CEO of St. Charles, said great thought went into the decision to reevaluate MA participation, and it was done only after years of concerns piled up not just at St. Charles, but at health systems throughout the country.
“The reality of Medicare Advantage in central Oregon is that it just hasn’t lived up to the promise,” he said in a press release. “A program intended to promote seamless and higher quality care has instead become a fragmented patchwork of administrative delays, denials, and frustrations. The sicker you are, the more hurdles you and your care teams face. Our insurance partners need to do better, especially when nurses, physicians and other caregivers are reporting high levels of burnout and job dissatisfaction.”
It's also worth noting that Memorial Hermann Health System, the largest hospital system in the Houston region, terminated its agreement with Humana's MA networks at the beginning of the new year. Memorial Hermann has not yet publicly cited why, other than saying the contract negotiations hit an impasse.
OK, but what’s the outcome of termination?
But what is it like on the other side of an MA termination? It hasn’t been so bad for some.
Hamilton Health Care System, a not-for-profit, fully integrated system of care serving the northwest Georgia region, has been out of network with MA for years.
“We are not currently in network with any Medicare Advantage plans. We would end up netting less than traditional Medicare because of denials and administrative hassles,” said Julie Soekoro, EVP and CFO at Hamilton Health Care System.
In addition to a lessened administrative burden, being out of network hasn’t affected Hamilton’s bottom line or patient experience.
“Since we are out of network, the MA plan should be paying us as if the patient were a regular Medicare patient, so it has not affected the patients adversely,” Soekoro said.
All the time and money spent on takebacks, pre-authorizations, and denials add up. Coupled with the aforementioned low reimbursement rates, CFOs can find it doesn’t make business sense to continue with the payer.
MA isn’t the only difficult payer, though; the challenge is universal.
For example, Hamilton Health Care has spent a lot of time going back and forth on a contract with a national payer that wanted to bring them in network, only for Hamilton to walk away from the negotiation table.
“After spending a great deal of time and effort modeling the contract, we learned the payer will require all diagnostic imaging business to go to a freestanding competitor, while building in very attractive looking rates for imaging,” Soekoro said. “This is misleading in that they never intended to allow their subscribers to come to us for imaging.”
“This was discovered incidentally by our contracting director, rather than fully disclosed by the payer,” she added. “Also, certain provider-favorable terms that we built into the language have mysteriously fallen out of the most recent version of the language.”
As stated, Hamilton walked away from that particular negotiation.
Another example comes from Berrett and his time at Texas Health Resources.
While Berrett didn’t specify the type of plan (MA or otherwise), the organization terminated a payer contract because its patients had significantly higher CMI, resulting in losses for their patients.
“The impact [of terminating the contract] was very positive for the hospital. We lost volume but improved margins,” he said. “The payer was able to promote a significantly lower premium for companies because their rates to the providers were so low. When we terminated the agreement, they could no longer sell lower premiums and their market share dwindled. They eventually retreated from the market.”
What does the future hold?
It’s worth noting that the trend of MA terminations is not a common occurrence with the nation's health systems—yet. In fact, several health systems expanded their own 2024 MA subsidiaries.
But that hasn’t stopped the critiques of the program from growing louder.
The Health and Human Services Department’s inspector general reported last year that some MA plans have denied coverage for care that should have been provided under Medicare's rules. On top of this, CMS and the Biden Administration have both proposed rules to address certain aspects of the plan’s requirements.
Even so, the payer/provider relationship is sure to remain heated in the coming year—even beyond MA.
“At the same time that community hospitals are struggling to stay out of the red, the national payers are reporting profits in the billions in their quarterly earnings reports,” Soekoro said.
“It feels to me like the payers became accustomed to taking in premiums during the volume downturns of the COVID years when patients shied away from seeking follow through on regular—and sometimes even urgent—healthcare needs,” she said. “Now the payers seem to be looking for ways to sustain those increased quarterly earnings.”
As for the providers, CFOs could have more leverage in negotiation talks than they think, but it requires willingness and preparation to pull levers that may be uncomfortable yet necessary for financial survival.
Dropping a payer is “absolutely an important strategy,” Berrett says. “Providers are becoming more capable in measuring the impact of the slow or rejected payments, and providers are looking at the actual cost of care by patient. Payers need to be aware that.”
There are two important considerations for providers, Berrett says.
“Are we able to collect our negotiated rates, and are the patients covered by this payer more expensive to treat?”
This year won't be easy for CFOs, but there are a few ways to set an organization up for success.
Stimulus funds are gone, median revenue growth is still slow, and expenses are continuing to increase due to a reliance on expensive external contract labor and increased wage costs.
Luckily there are many ways hospital and health system CFOs can make sure they are setting their organization up for success, and Brett Tande, CFO of Scripps Health, recently shared four of them with HealthLeaders:
It’s clear that labor challenges—and the cost of that labor—will continue to be a prominent concern for healthcare organizations. As a handful of various industries have participated in massive strikes in 2023, the trend in healthcare is likely to continue.
That being said, hospital CEOs and CFOs should anticipate—and prepare—for some heightened labor negotiations this year.
The Kaiser union’s disagreement over across-the-board raises in 2023 was a significant financial concern, however, not uncommon. Hospital leaders must carefully assess the impact of wage increases on their budgets, especially when facing demands for higher pay. Balancing fair compensation for healthcare workers with financial sustainability is going to have to be top priority.
Bringing down labor costs is an area of focus for many hospital CFOs, but not at the risk of creating staffing turnover. Cost savings can be undercut by the resources required to replace workers, including interviewing candidates and training new employees.
New workers are also less productive in their initial transition period than established staff, which leads to less revenue. These factors should be considered when hospital leaders weigh the threat of losing workers by not meeting wage demands.
Wage laws
Even if your staff is happy, that doesn’t mean you won’t be required by law to increase wages across the board.
Take California for example.
California Governor Gavin Newsom signed a new law that will gradually raise healthcare workers' hourly minimum wage to $25, a bill that has an estimated price tag of $4 billion for the 2024-25 fiscal year.
But, that estimated $4 billion price tag is just at the state level and doesn't necessarily include the costs for private organizations or those in the non-profit healthcare world, so CFOs in California in particular really need to strategize for this unknown added cost.
As for CFOs outside of California, while wage increases weren’t as high as California, many states saw a wage increase on January 1.
What more can CFOs do?
Organizations need to recruit and retain talent in house and on a budget.
Gone are the days when CFOs of smaller (and even large) organizations can throw money at the problem—i.e., salary increases and bonuses—to attract and keep talent, especially when a hospital 20 minutes down the road can pay their staff much more for the same job.
So, what can leaders do to bolster the workforce while keeping expenses low? Placing an emphasis on culture and scheduling flexibility is a great place to start.
Here are several budget-friendly strategies that I have complied from talks with CFOs across the country that other leaders can employ in 2024:
Asses your employee benefits and perks: Offer a comprehensive benefits package that includes health insurance, retirement plans, and additional perks such as flexible work schedules, wellness programs, or tuition reimbursement.
Prioritize training and staff development: Provide budget-neutral ongoing training and professional development programs. Staff value opportunities to enhance their skills and advance their careers, so offering educational support, workshops, or mentorship programs can demonstrate your commitment to their growth. Cross-training employees in various roles within the organization is also a great way to enhance schedule flexibility and help bridge staffing gaps.
Form recognition or reward programs: Implement a robust recognition and rewards program to acknowledge and celebrate employee achievements. Non-monetary rewards, like public recognition, awards, or personalized thank-you notes, can boost morale and motivation.
Emphasize work-life balance: Promote work-life balance by offering flexible scheduling, remote work options (where feasible), and paid time off. Emphasizing the importance of a healthy work-life balance can help attract and retain staff.
Implementing wellness initiatives to support employee health and reduce burnout can also help in this area too. These programs can include stress reduction workshops, access to fitness facilities, and mental health support.
Create career advancement opportunities: Create a clear career path within the organization. Staff are more likely to stay when they see opportunities for advancement. Encourage internal promotions and provide training for leadership roles.
Streamline existing technology: Be creative in ways to bolster the technology and tools you already have to streamline workflows and reduce administrative burdens. This can improve staff efficiency and allow them to focus more on patient care.
Prioritize community involvement: The attendees agreed that many healthcare professionals—especially those in more rural areas—are motivated by a sense of purpose and making a difference in the community, so highlight your hospital's role within the community and engage employees in community service or outreach programs.
Incorporating a combination of these strategies can help small and medium-sized hospitals strengthen their workforce, improve staff satisfaction, and remain competitive in the healthcare industry without solely relying on salary increases.
In a field of 2,644 short-term, acute care non-federal US hospitals, Forbes says there were 100 organizations—which represent teaching and community hospitals of various sizes—that stood apart and serve as guides for the broader industry.
This list measured patient outcomes and experience, operational efficiency, financial health, and community impact, to see which organizations came out on top. And according to PINC AI’s analysis, there’s much to gain in following their lead.
“If all hospitals performed at the same level as the 100 Top Hospitals, more than 272,000 additional lives would be saved in the hospital and more than 432,000 additional patients would be spared complications as a result of care. $15.7 billion in inpatients costs would be avoided,” the report says.
While the entire list is available in the report, let’s take a look at the top 10 major teaching hospitals and large community hospitals:
Top Major Teaching Hospitals:
1. Baylor Scott & White Medical Center - Temple
Location: Temple, Texas Clinical outcomes:★★★★★ Operation efficiency: ★★★★★ Patient experience:★★★★ Financial health: ★★★★★ Community health survey performance: 100% Total number of years on 100 Top list: 13 Website
2. Trinity Health Ann Arbor Hospital
Location: Ypsilanti, Mich. Clinical outcomes: ★★★★★ Operation efficiency: ★★★★★ Patient experience: ★★★★★ Financial health: ★★★★ Community health survey performance: 100% Total number of years on 100 Top list: 13 Website
2. Baylor University Medical Center
Location: Dallas Clinical outcomes: ★★★★★ Operation efficiency: ★★★★ Patient experience: ★★★★★ Financial health: ★★★★★ Community health survey performance: 100% Total number of years on 100 Top list: 5 Website
4. St. Luke's University Hospital - Bethlehem
Location: Bethlehem, Penn. Clinical outcomes: ★★★★★ Operation efficiency: ★★★★★ Patient experience: ★★★★ Financial health: ★★★★★ Community health survey performance: 100% Total number of years on 100 Top list: 11 Website
5. University of Utah Hospital
Location: Salt Lake City Clinical outcomes: ★★★★★ Operation efficiency: ★★★★★ Patient experience: ★★★★★ Financial health: ★★★★ Community health survey performance: 100% Total number of years on 100 Top list: 6 Website
6. NYU Langone Health - Tisch Hospital
Location: New York City Clinical outcomes: ★★★★★ Operation efficiency: ★★ Patient experience: ★★★ Financial health: ★★★★ Community health survey performance: No survey data Total number of years on 100 Top list: 2 Website
7. Vanderbilt University Medical Center
Location: Nashville, Tenn. Clinical outcomes: ★★★★★ Operation efficiency: ★★★★★ Patient experience: ★★★★★ Financial health: ★★★ Community health survey performance: No survey data Total number of years on 100 Top list: 15 Website
8. Pennsylvania Hospital
Location: Philadelphia Clinical outcomes: ★★★★★ Operation efficiency: ★★★★★ Patient experience: ★★★★ Financial health: ★★ Community health survey performance: No survey data Total number of years on 100 Top list: 2 Website
9. UCHealth University of Colorado Hospital
Location: Aurora, Colo. Clinical outcomes: ★★★★★ Operation efficiency: ★★★★ Patient experience: ★★★★ Financial health: ★★★★★ Community health survey performance: 100% Total number of years on 100 Top list: 9 Website
10. Penn Presbyterian Medical Center
Location: Philadelphia Clinical outcomes: ★★★★★ Operation efficiency: ★★★★ Patient experience: ★★★★★ Financial health: ★★★★ Community health survey performance: 100% Total number of years on 100 Top list: 5 Website
Top Large Community Hospitals
1. St. David's Medical Center
Location: Austin, Texas Clinical outcomes: ★★★★★ Operation efficiency: ★★★★★ Patient experience: ★★★★★ Financial health: ★★★★★ Community health survey performance: 100% Total number of years on 100 Top list: 14 Website
2. St. David's North Austin Medical Center
Location: Austin, Texas Clinical outcomes: ★★★★★ Operation efficiency: ★★★★ Patient experience: ★★★★ Financial health: ★★★★★ Community health survey performance: No survey data Total number of years on 100 Top list: 5 Website
3. Parkridge Medical Center
Location: Chattanooga, Tenn. Clinical outcomes: ★★★★★ Operation efficiency: ★★★★★ Patient experience: ★★★★ Financial health: ★★★★★ Community health survey performance: 25% Total number of years on 100 Top list: 5 Website
4. Sharp Memorial Hospital
Location: San Diego Clinical outcomes: ★★★★★ Operation efficiency: ★★★★★ Patient experience: ★★★★★ Financial health: ★★★★★ Community health survey performance: 100% Total number of years on 100 Top list: 2 Website
5. Houston Methodist Sugar Land Hospital
Location: Sugar Land, Texas Clinical outcomes: ★★★★★ Operation efficiency: ★★ Patient experience: ★★★★★ Financial health: ★★★★★ Community health survey performance: No survey data Total number of years on 100 Top list: 5 Website
6. Cape Coral Hospital
Location: Cape Coral, Fla. Clinical outcomes: ★★★★★ Operation efficiency: ★★★★★ Patient experience: ★★★ Financial health: ★★★★★ Community health survey performance: 100% Total number of years on 100 Top list: 4 Website
7. Saint Mary's Regional Medical Center
Location: Reno Clinical outcomes: ★★★★★ Operation efficiency: ★★★★★ Patient experience: ★★ Financial health: ★★★ Community health survey performance: 100% Total number of years on 100 Top list: 4 Website
8. Medical City Plano
Location: Plano, Texas Clinical outcomes: ★★★★★ Operation efficiency: ★★ Patient experience: ★★★★ Financial health: ★★★★★ Community health survey performance: No survey data Total number of years on 100 Top list: 2 Website
9. Chippenham Hospital
Location: Richmond Clinical outcomes: ★★★★★ Operation efficiency: ★★★★ Patient experience: ★★★ Financial health: ★★★★★ Community health survey performance: 75% Total number of years on 100 Top list: 3 Website
10. Olathe Medical Center
Location: Olathe, Kan. Clinical outcomes: ★★★ Operation efficiency: ★★★★★ Patient experience: ★★★★ Financial health: ★★★★★ Community health survey performance: No survey data Total number of years on 100 Top list: 2 Website
Margin declines, expense growth, and an impending "labordemic" has been spelling trouble for non-profit hospitals looking to claw their way to financial relief.
Median operating and operating EBITDA margins for non-profit hospitals declined significantly from fiscal year 2021 to 2022, Fitch Ratings said, and this decline is primarily due to persistent high labor costs and the inelastic nature of hospital revenue.
In fact, with stimulus funds tapering off, median revenue growth slowed and expenses increased due to a reliance on expensive external contract labor and increased salary and wage costs.
So, what can CFOs of non-profit hospitals and health systems do to fight back?
CFOs need to place their focus on operational effectiveness, Brett Tande, CFO of Scripps Health, a $4.3 billion not-for-profit integrated health system in San Diego, California, told me in November.
“Consistent with what we've been showing in our quarterly results throughout 2023, we're probably going to lose about $30 [million] to $40 million in our next earnings report,” Tande says.
“One of the biggest items that we need to focus on is getting back to profitability,” he says.
Why has profitability been a challenge for Scripps? Aside from labor costs and hardships from the pandemic, the system has been undergoing various construction projects even prepandemic. But nonetheless, profitably is what pays for these updates.
“What pays for that is that positive operating cash flow that we need,” he says. “And when it's depressed, you've got to see those debt levels come up. And that's what we've been seeing over the last couple of years. And I think for in 2024, we'll see that more as well.”
That being said, getting that profitability back to a level that can support the organization will be very important, Tande said, “so, I will be working on that.”
The question then becomes, how do you do that?
Tande said the pandemic was very challenging for Scripps, not only financially but obviously for its staff as well.
Now that we are on the other side of the pandemic, Scripps’ focus is on operational effectiveness, and Tande says the last year or two have been really promising.
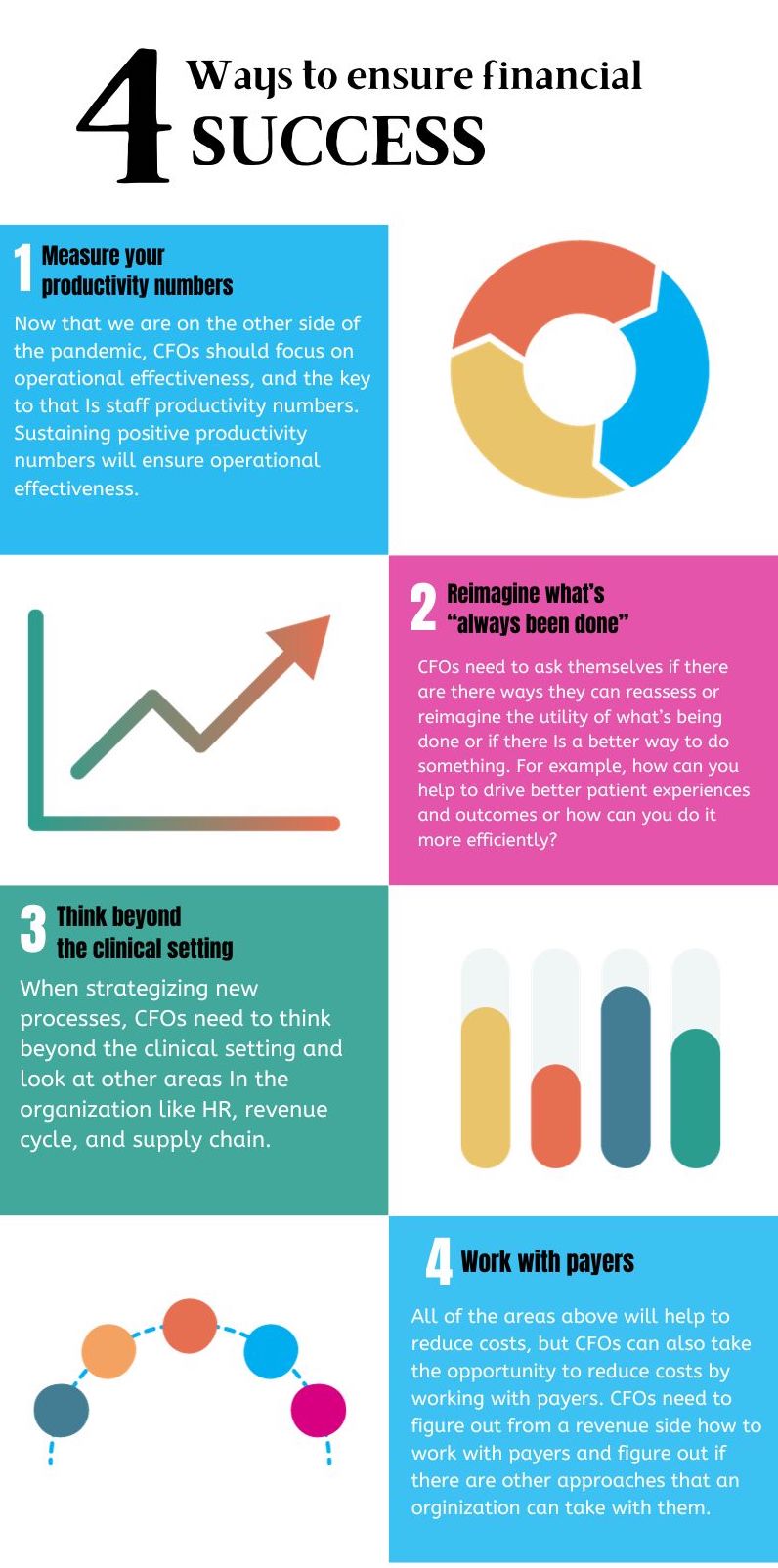
“Our productivity numbers now look great throughout the organization and we're really just trying to sustain that,” he says. “We think that has a lot of value.”
Aside from maintaining productivity, reimagining what’s “always been done” is necessary as well.
“Are there ways we can reassess or reimagine the utility of what we're doing or is there a better way to do something?” Tande pondered. “How can we help to drive a better patient experience and outcome or how can we do it a little bit more efficiently?”
That's the approach they have to take, he says.
“And again, it's not just in that clinical setting,” Tande says. “Reimagining operations has to be done throughout the organization. It could be in HR, revenue cycle, supply chain, or otherwise, but we need to try to be able to reduce our costs.”
When reducing costs, “there are a lot of irons that we have in the fire across the organization,” Tande says.
And, like most organizations, working with payers isn’t off the table when looking to reduce costs.
“We have to figure out from a revenue side how to work with payers and figure out if there are other approaches that we can take with them,” he says. “Which is something that the entire industry needs to do.”












3474.jpg?itok=5lSCtI-9)

