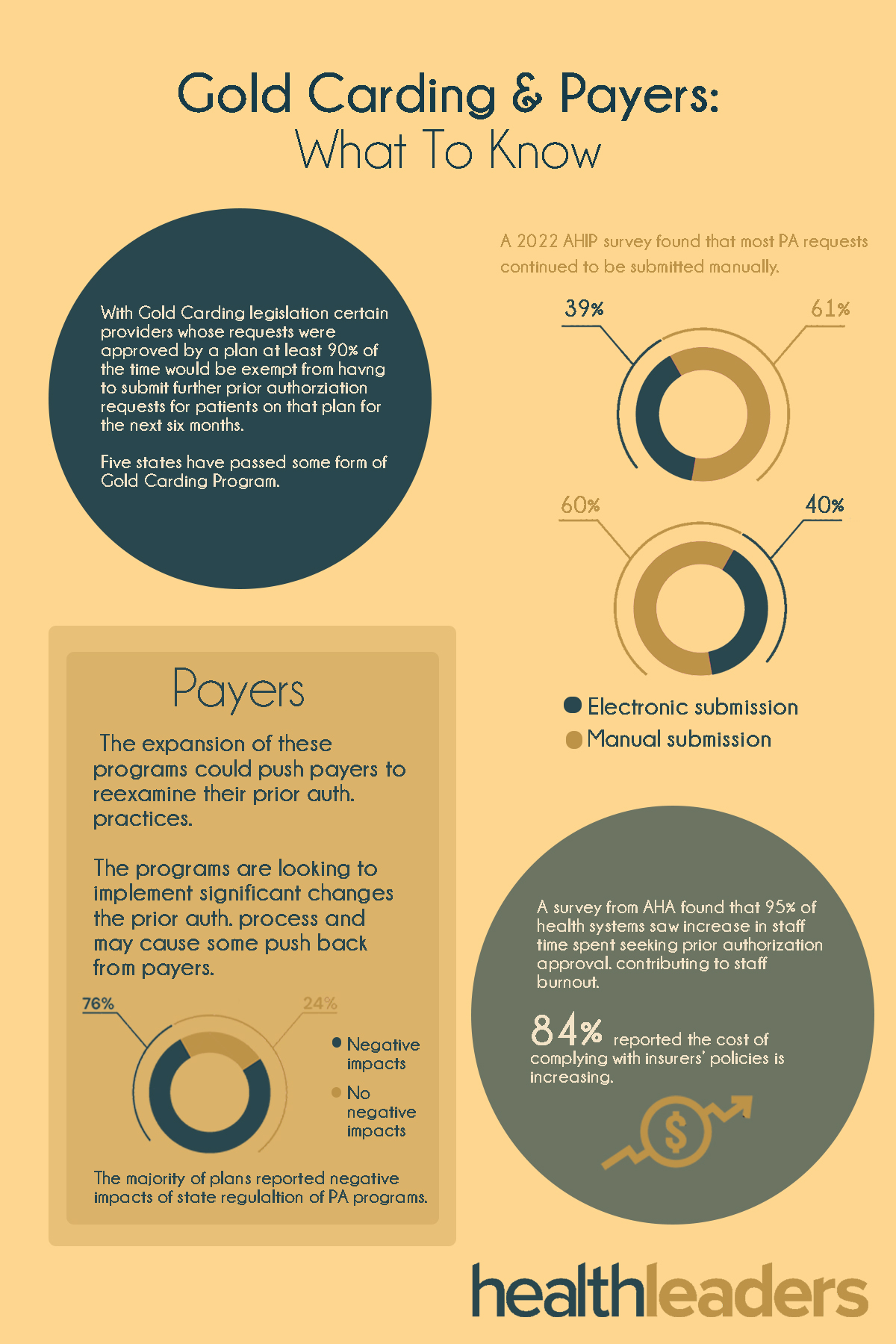
Gold Carding is expanding across the country with several states already implementing the legislature in some way.
The states are fighting back against prior authorization woes. In Janaury, the Biden adminstration announced new rules to help streamline the PA process, but states are taking it even further with Gold Carding legislation. Studies have shown that prior authorization has been a big pain point for health systems, and is contributing to things like worker burnout and higher costs.
Check out the infographic below to see how prior authorization delays and denials are affecting health systems, as well as what this legislation means for payers.
How do you balance financial priorities with quality patient care?
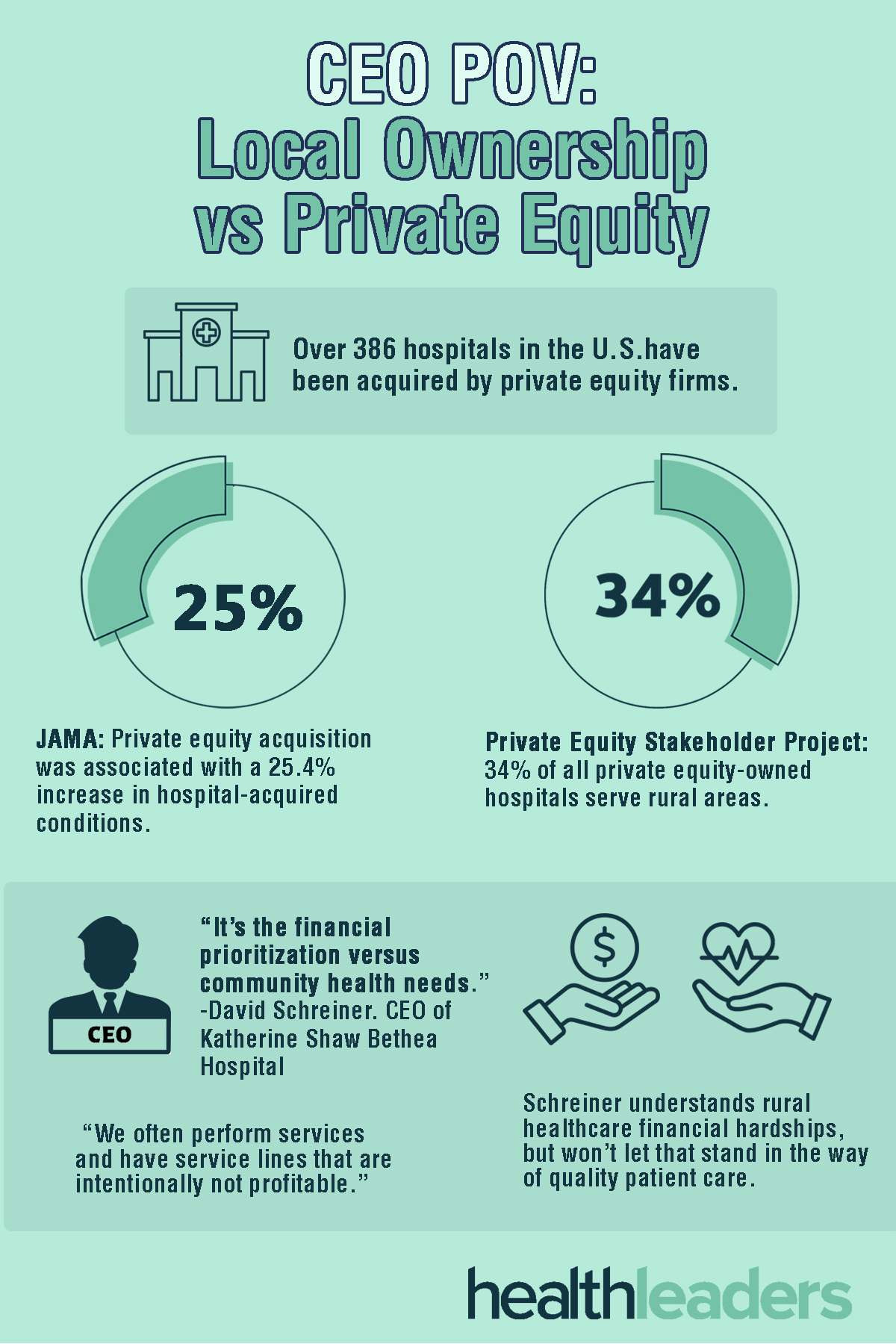
Private equity accounts for over 30% of all hospitals in rural areas, which can make a big difference in how an organization operates. How do you balance financial priorities with quality patient care? For one CEO, it’s a no-brainer.
David Schreiner is the CEO of Katherine Shaw Bethea Hospital in Dixon, Illinois, and he sees the friction here. But he also knows that quality patient care is not an item he will compromise on.
“We're an independent rural hospital. We have no ownership, no one is receiving dividends or investment returns from our organization,” he said in an interview with HealthLeaders.
This is the second setback in what would be a $2.5B sale.
Less than 12 hours before regulatory hearings were set to take place, Blue Cross halted the sale to Elevance, for the second time this year. Citing regulatory and stakeholder concerns, BCBS has paused the sale for what would have been the biggest healthcare deal in the state’s history. BCBS operates in all 50 states and their Louisiana operation is the state’s largest insurer with 1.9 million members.
"It is clear that our stakeholders need more time and information to understand the benefits of the changes we have proposed," Blue Cross said in a statement. "This is why we have decided to again pause the process in our proposed transaction with Elevance Health.”
For the sale to go through BCBS would have to reorganize itself as a for-profit entity, which isn’t sitting well with state regulators. Worried the deal could present anti-competitive issues and raise premiums, state regulators also question how the proceeds would be split amongst policyholders.
BCBS proposed a reorganization plan back in December last year, but was unsuccessful in swaying stakeholders.
“I’m glad it was shelved,” Senate Insurance Committee Chairman Kirk Talbot, R-River Ridge said. “That process had a lot of problems.”
BCBS has argued for the deal, stating that it would be the best way to navigate a rapidly changing healthcare landscape. The payer says the deal could allow more financial resources and flexibility to operate and expand in Louisiana, and would better member experience and benefits.
In order to go through, the deal would require approval from Louisiana’s insurance commissioner and two-thirds of BCBSLA policyholders.
The sale was also largely unpopular amongst healthcare and physicians’ groups, the state medical society even sending an open letter to policyholders urging a “no” on the deal.
Meanwhile, Elevance says it is supportive of BCBS’s decision to withdraw the plan at this time. "We will continue to meaningfully engage community members who are truly interested in better health outcomes and more affordable health care," Elevance officials said. "We remain committed to this partnership.”
Indiana-based Elevance, which operates BCBS plans in 14 states, is one of the largest insurers in the country. With its own telehealth platforms, pharmacy benefits manager and specialty physician practices, BCBS was hoping these items would help it provide better services to its Louisiana members.
If the sale is completely scraped, Elevance could scope out other potential partners.
However, during two legislative hearings about the acquisition several questions were raised concerning Elevance. Concerns over whether or not Elevance would be able to retain the 2,500 Louisiana based employees, as well as confusion over which policy holders were allowed to vote on the sale were two major pain points.
Stakeholders that have been closely following the controversial deal seemed divided on whether or not BCBS would come back with another revised plan.
The deal has been controversial from the beginning, but will it be able to gain the lawmaker support it needs to proceed in the future?
Federally qualified health centers (FQHCs) are using digital health tools to improve patient experience and care coordination.
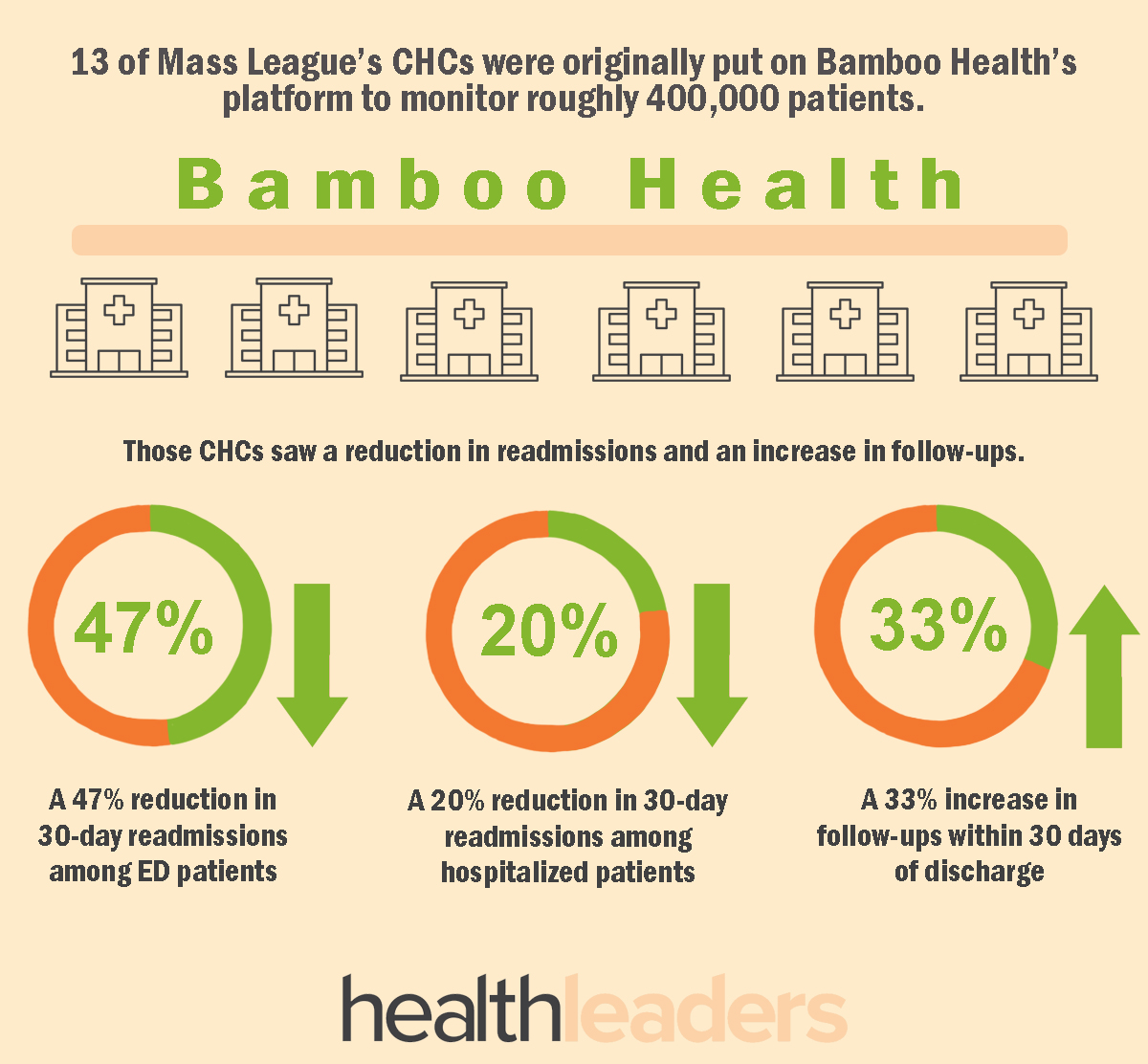
FQHCs, RHCs (rural health centers) and CHCs (community health clinics) serve millions of Americans as their sole form of healthcare access. Through Telehealth and digital health tools, providers are addressing care issues that typically end up creating higher costs and poorer patient outcomes. The tech is ultimately helping providers improve chronic care management and address social determinants of health.
For example, the Massachusetts League of Community Health Centers, which serves 52 CHCs, 300 sites and 1 million patients, is using an RSA grant to implement a technology that keeps track of when and where patients receive care. The platform, developed by Bamboo Health, sends real-time notifications to care teams when a patient visits another provider outside of the system. This then enables the care team to access admission, discharge and data transfers.
Since the pandemic unions and general workforce unrest have been rising.
CEOs must be prepared to deal with components in their organization that can spark unionization. Some top reasons for union formation are burnout, administrative burden, and understaffing. Union or no union, CEOs must know where their organizations' vulnerabilities lie, how they can approach the issues that are present, and where and how they can be flexible in their solutions.
A number of states are looking to Medicaid for coverage.
As of March 2023 16.9M people were disenrolled from Medicaid, and rates for disenrollment have varied widely across each state. Meanwhile, more states are pushing for Medicaid expansion. Florida, Georgia, North Carolina and Texas have recently made some moves in this space to acquire coverage.
CMS is cracking down on AI use in Medicare Advantage.
Medicare Advantage (MA) insurers can use AI and algorithms to assist in making coverage decisions, but CMS is warning the insurers that they must follow the agency’s internal benefits requirements and nondiscrimination rules under the ACA and lawfully deny care.
This recent warning aimed at MA insurers addressed concerns surrounding coverage criteria and utilization management requirements from CMS’ final rule policy that detailed policy and technical changes to MA; the rule was originally issued last April.
"We are concerned that algorithms and many new artificial intelligence technologies can exacerbate discrimination and bias," CMS wrote in the memo. "MA organizations should, prior to implementing an algorithm or software tool, ensure that the tool is not perpetuating or exacerbating existing bias, or introducing new biases."
What exactly is CMS saying?
In the memo CMS highlights a few important items, including their clarification between an algorithm and an AI model.
It defined AI as: “a machine-based system that can — for a given set of human-defined objectives — make predictions, recommendations or decisions influencing real or virtual environments,” and algorithms as technology that “can imply a decisional flow chart of a series of if-then statements."
CMS detailed that while algorithms can aid in predicting the length-of-stay for post-acute service, they cannot make the decision of terminating coverage. Regarding inpatient admissions, the agency stated that algorithms and AI alone cannot be used as a reason to deny admission or downgrade an observation stay.
CMS also stated that while payers may use algorithms to assist in coverage decisions, they must ensure the tech is compliant with the agency’s coverage decision requirements. MA payers cannot make decisions based on a larger data set, and decisions must be based on an individual patient’s medical history, provider recommendations, and clinician notes.
How did we get here?
In 2023 the federal government told MA insurers repeatedly that they cannot use AI to deny care. We saw three giants Cigna, Humana and UnitedHealthcare faced with lawsuits for allegedly using AI to wrongfully deny claims.
The issue has even garnered attention from senators.
At a recent hearing Senator Elizabeth Warren called out MA insurers for wrongfully using AI to profit off of deny claims. “Without significant guardrails in place, these (AI) algorithms will continue to harm patients while padding the private insurers’ profits,” said Warren.
Senator Warren questioned Michelle M. Mello, JD, PhD, professor of health policy and law at Stanford University, about what measures CMS should take to ensure that private insurers are not leveraging AI tools to unlawfully deny care.
“CMS plans to beef up its audits in 2024 and specifically look at these denials. That seems extremely important. But beyond that, I think additional clarification is needed to the plans about what it means to use algorithms properly or improperly,” Mello stated. “For example, for electronic health records, it didn’t just say ‘make meaningful use of those records,’ it laid out standards for what meaningful use was.”
Senator Warren commented: “Until CMS can verify that AI algorithms reliably adhere to Medicare coverage standards, by law, then my view on this is: CMS should prohibit insurance companies from using them in their MA plans for coverage decisions. They’ve got to prove they work before they put them in place.”
MA payers must ensure they stay on top of these guidelines to avoid future scrutiny over denials and AI use. CMS has also created a website as an AI resource for insurers.
AI is just one of the many items recently shaking up the MA space. In addition to evolving tech, check out three other items MA payers will need to stay on top of this year.
The New York City-based health system was fined $4.75 million after a federal investigation found that a former employee and stolen patient data from the EHR.
Montefiore Medical Center has agreed to pay a $4.75 million fine for failing to secure patient data.
According to the HHS, Montefiore received a tip in 2015 from federal officials about a data breach. An investigation by health system officials found that since 2013 a former employee had been accessing the data of more than 12,000 patients through the health system’s electronic medical record system. The data included names, addresses, social security numbers, and confidential medical records.
Montefiore filed a breach report with HHS, prompting the federal investigation.
Investigators found that the health system failed to “analyze and identify potential risks and vulnerabilities to protected health information, to monitor and safeguard its health information systems’ activity, and to implement policies and procedures that record and examine activity in information systems containing or using protected health information.”
By failing to properly monitor its EHR, the investigation reported, Montefiore was unable to stop the cyberattack or even detect it until years later.
Since the investigation and arrest of the former employee, who was charged with three felonies, Montefiore officials say they have taken steps to improve security and protect patient data. This includes expanding monitoring capabilities around patient information and implementing additional technical safeguards to protect all electronic records.
A Montefiore spokesperson told HealthLeaders in an e-mail that they have also increased training and outreach to staff to reinforce privacy and security standards, reminding staff that patient privacy is a basic right.
“With healthcare systems across the country continuing to be targets for data breaches and other malicious cyberattacks, we take our responsibility to protect patient information very seriously and remain committed to ensuring safety protocols and cybersecurity safeguards are always maintained to protect our patients' privacy,” the spokesperson said.
Cybersecurity attacks on healthcare systems are becoming more common. According to HHS, from 2018-2022 there was a 93% increase in large data breaches reported to OCR, and a 287% increase in large breaches using ransomware. In 2023 alone two new records were set: the most reported data breaches (725) and the most breached records (133 million).
“Unfortunately, we are living in a time where cyberattacks from malicious insiders are not uncommon,” OCR Director Melanie Fontes Rainer said in the HHS press release on the Montefiore investigation. “Now more than ever, the risks to patient protected health information cannot be overlooked and must be addressed swiftly and diligently.”
“This investigation and settlement with Montefiore are an example of how the health care sector can be severely targeted by cyber criminals and thieves—even within their own walls,” she added. “Cyber-attacks do not discriminate based on organization size or stature, and it’s incumbent that our health care systems follow the law to protect patient records.”
In March 2023 the Biden Administration released a National Cybersecurity Strategy, and HHS followed this with a healthcare-specific plan indicating that the agency would play a more active role in helping health systems become more secure.
The plan highlights four main guidelines that HHS will follow to help ensure the security of health systems. The agency plans to:
Establish voluntary cybersecurity performance goals for the healthcare sector;
Provide resources to incentivize and implement these cybersecurity practices;
Implement an HHS-wide strategy to support greater enforcement and accountability; and
Expand and mature the one-stop shop within HHS for healthcare sector cybersecurity.
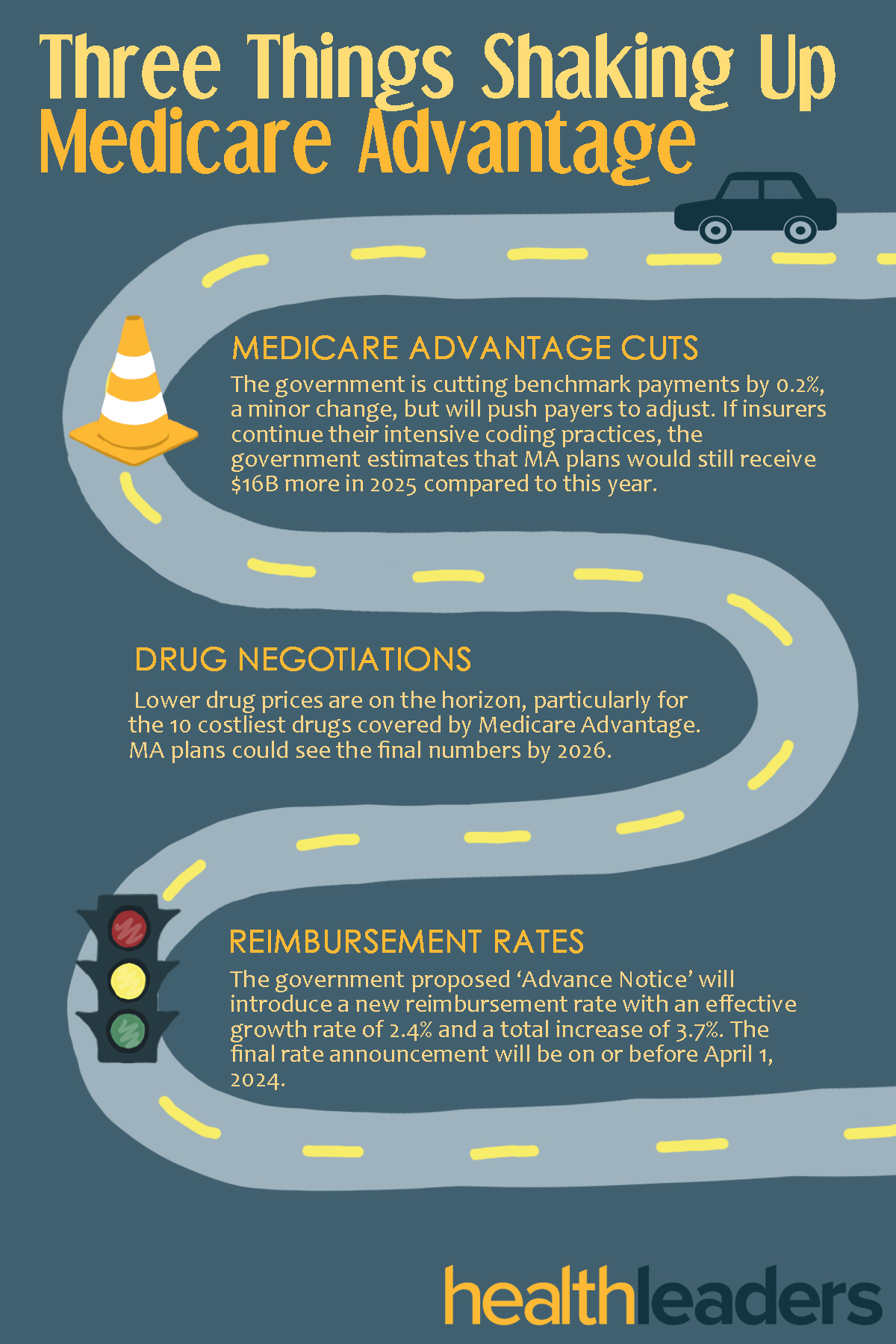
Medicare Advantage has seen a lot of turbulence recently.
With everything happening in the Medicare space there are bound to be a few items that will shake up the scene for payers this year. With questions floating around like ‘is the Medicare gold rush slowing down?’, some insurers may be questioning whether or not MA is as profitable as it used to be. There are important factors to consider when looking at how MA will progress over the next two years, here are three that are bound to shake up the Medicare Advantage space soon.
What the $3.7 billion dollar deal means for each company.
The deal is just about sealed. Cigna is ditching its Medicare business in a sale to Health Care Service Corporation (HCSC) for around $3.7B, set to close in early 2025.
HCSC will acquire Cigna’s Medicare Advantage, Part D, Supplemental Benefits, and CareAllies businesses, which in total currently provide about $7.9B in revenue for the giant. Cigna’s Medicare business currently serves 3.6 million members, with close to 600,000 members in MA plans, over 450,000 on Medicare Supplement plans, and 2.5 million with Medicare Part D. Its CareAllies business serves approximately 450,000 patients. As part of the deal, Cigna’s Evernorth Health Services subsidiary entered into a four-year agreement with customer-owned health insurer HCSC to continue to provide pharmacy services to Medicare plans if the deal officially closes.
Did We Expect This?
There were rumors of Cigna mulling the sale back in November, and we even saw Elevance enter into somewhat of a bidding war with HCSC for Cigna’s Medicare businesses in December. We all knew this acquisition was in the cards, but did we expect HCSC to prevail over Elevance? Looking just at size and revenue, Elevance is raking in over triple that of HCSC, $170B (2023) vs $54B (2022), and it seemed Elevance would take the pot. HCSC is also not publicly traded like Elevance, limiting it to a cash-only offer. Perhaps a quick cash offer is what Cigna was looking for in this deal; the sale comes at a time when government scrutiny of Medicare is high. Cigna pushed through with this sale despite their failed merger with Humana in December.
What It Means For HCSC
This acquisition marks a big transformational step in HCSC’s growth, taking it from a regional to a national insurer. With license to provide BCBS plans in five states, HCSC employs over 27,000 people and serves 18.6 million members.
In a press release HCSC CEO Maurice Smith said that this sale will allow the insurer not only to quickly scale, but also evolve its product portfolio.
"This acquisition supplements our growth strategy in the large and growing Medicare marketplace and will bring many opportunities to HCSC and its members—including a wider range of product offerings, robust clinical programs, and a larger geographic reach," Smith said.
What It Means For Cigna
Cigna seems to be making particularly strategic moves with this sale. The insurer acquired its Medicare sector in a $3.8B acquisition of HealthSpring back in 2011. But the majority of Cigna’s revenue doesn’t stem from their Medicare business, but rather their commercial and pharmacy benefits divisions where it spent $52B in a purchase of Express Scripts in 2018.
CEO David Cordani of The Cigna Group said that this HCSC sale will allow the company to focus on growth targets.
"This decision is aligned with our highly disciplined approach to managing our portfolio and allocating resources toward growth opportunities in our Evernorth Health Services and Cigna Healthcare portfolios," Cordani said in the press release. "While we continue to believe the overall Medicare space is an attractive segment of the healthcare market, our Medicare businesses require sustained investment, focus, and dedicated resources disproportionate to their size within The Cigna Group's portfolio."
While this is a big move for HCSC’s expansion and portfolio evolution, will the company be able to retain all of Cigna’s Medicare members? Going forward in the current Medicare landscape is uncertain, and the “Medicare Gold Rush” we saw at the start of last year has teetered off. HCSC serves more than 22 million members across the country and will be adding 3.6 million more if the sizable deal goes through.








.jpg)