Could a sales tax solve hospitals' financial crisis?
Denver Health is turning to its city council as it faces a financial crisis.
The nonprofit hospital is working with members of the city council to implement a 0.34% sales tax increase that would help pay for uncompensated care. If approved, the tax will be added to the ballot in November.
Denver Health has been struggling with uncompensated care costs for a while. In 2020, the hospital lost $60 million from uncompensated care costs, and saw that number double to $120 million in 2022. Last year its uncompensated care costs soared to $136 million, with $35 million of that sum coming from patients who live outside the city. Over half—65%—of Denver Health’s patients are covered by Medicaid or are uninsured.
Medical Costs Hitting Nonprofits
Denver Health is one of many nonprofit health systems across the country feeling the effects of soaring costs. Nonprofits seemed to be doing okay after the pandemic, with one study showing 73% of nonprofit hospitals and health systems had at least “strong” days of cash on hand in 2022.
Although margins have increased, and some nonprofits have had luck pivoting elsewhere to increase operating margins, some are still dealing with rising labor costs. Labor expenses continue to weigh down hospitals and with nonprofits unable to cut services, cost caps are coming into play.
However, cost caps may even be further damaging to nonprofits. A report from Fitch Ratings shows how state benchmarks could hurt nonprofit revenue and operating margins during a time when operators are combating rising expenses.
Denver’s Dilemma
The proposed tax would increase Denver's sales tax to over 9%, with the tax collection capped at $70 million. According to NBC affiliate KUSA, a city council member has advanced the proposal, which still requires full council approval before it gets on the ballot.
According to the Denver Gazette, this tax would make Denver the highest-taxed major city in the wider metro area, and some council members worry that Denver voters may recoil at the prospect of a tax hike.
According to the report, earlier this year Denver Health CEO Donna Lynne put pressure on state and federal policymakers to pay for the uncompensated care costs. In March, the state accelerated $5 million to the hospital when state health care leaders warned that the hospital was nearing a financial “death spiral”
According to Lynne, the sales tax would ensure that patients outside the city are helping to cover the payments.
"There is a possibility that there would have to be service reductions, if we are not successful in all of those fronts," she said, according to the report.
The gap between highest and lowest performing hospitals shrank this year.
Nonprofit hospital margins jumped to 4.3%, up 33% year over year, according to findings from a KaufmanHall report released.
In addition to the improved margins for the 1,300 hospitals analyzed in the report, the gap between the lowest and highest performing hospitals has narrowed. Those that performed the best saw a margin of 28.9%, while the worst performing hospitals came in at -16.1%.
“While hospital margins have demonstrated improvement over the last several years, growth has slowed in the last few months and may be settling on a new normal. A closer look at hospital performance at the individual level shows an increased divide between higher performing and lower-performing hospitals,” said report author and senior vice president of data and analytics Erik Swanson in the report.
Month over month operating margins were up 7%, and year to date they soared to 21% higher than in 2023. The operational cash profit margin year to date was also up 14% compared to the same period last year.
In April, net operating revenue per calendar day increased to 9% year to date, 5% year to date in March. Year over year in April inpatient revenue jumped to 12%.
Data from the KaufmanHall report showed three notable items:
In April outpatient revenue increased 10% year over year and average length of stay decreased 4%. Emergency department visits also increased up to pre-pandemic levels.
The Big Picture
Last year labor costs and inflation brought major cash shortages to many hospitals. Margins from 2020 indicate that federal support was vital throughout the pandemic in order for hospitals to remain financially viable.
In search of cost savings, many hospitals turned to supply chain optimization and the delay of new tech implementations. From one study, many hospitals and health systems cited low payer reimbursement as the top cause for low operating margins.
“Recovering from the pandemic, we have seen a slight overall improvement in average operating margins over the past three years,” said HFMA Chief Partnership Executive Todd Nelson in a press release.
Bouncing Back From 2023
A previous study by Deloitte found that operating margins reached an eight year low of -0.8% in 2023.
Health systems are the “lifeblood” of an innovative health system, the report concludes. Profits are important to fund the mission of a health system and enable it to better serve the community. Leaders should focus on their fiduciary responsibility to support health systems long term.
The health system is one of many nonprofits seeing strong gains coming out of the first quarter.
Advocate Health reported a first-quarter operating income of $103.7 million, according to financial reports released last month. This is compared to the system’s earnings of $10.4 million during the same period in 2023.
The health system’s first quarter revenue increased 7.8% year over year to $8.1 billion, but expenses closely followed, growing 6.6% to $8 billion. The 67-hospital system saw labor costs increase 6.7% to $4.7 billion, while supply and drug costs increased 12.5% to $1.7 billion.
After the addition of nonoperating items like investment returns, the system saw a net income of $682.6 million after the first quarter, up from $578.7 million from its first quarter in 2023.
The total sum for unrestricted cash and investments was $21.8 billion and long-term debt was $7.4 billion.
Where the Nonprofit Found Strength
Major nonprofit health systems have seen consistent higher volumes and revenues, specifically for second quarter results, but not all have fared so well. For instance, Providence (the sixth largest nonprofit) reported a $202 million operating loss (-2.8% operating margin) in its second quarter last year.
In 2022, about 73% of nonprofit hospitals and health systems had at least “strong” days of cash on hand, but about one in ten (9%) had “vulnerable” or “highly vulnerable” levels, according to an S&P report. Advocate Health brought in about $27 billion in annual revenues during 2022, according to the system’s financial reports.
According to a Kaiser Family Foundation report, “the value of financial investments among nonprofit hospitals and health systems have likely stabilized or increased with 2023 market improvements.”
Based on financial reports it’s likely that pandemic relief funds lent a hand in these non-recurring operating revenues. Totals jumped from $13 million in 2019 to $29 billion among nonprofit health systems, and fell down to $8 billion in 2022, according to KFF news.
The improvement of operating margins in 2023 is perhaps due to decreases in labor expenses and increases in volume and reimbursement rates, but even so, these margins tend to remain below pre-pandemic levels.
Advocate Health, born out of the partnership of Advocate Aurora Health and Atrium Health, saw its earnings soar upwards nearly a billion halfway through its first year with an operating margin of 0.6% and a whooping $938.4 million from investments.
A lot of CFO shuffling has happened since the beginning of 2024.
This year new CFOs are stepping into new roles and expanding their titles at several health systems all over the country. Studies show that healthcare CFO tenures last an average of 4.7 years.
Here’s a list of five recent CFO moves to know:
Allina Health, a Minneapolis-based health system, moved Doug Watson to CFO. Since January Watson was the system's interim finance executive.
New York City-based Montefiore Health System executive vice president and CFO Colleen Blye expanded her role to chief business officer.
Nikki Hutchinson succeeded Tim Rieger as CFO of Cincinnati-based Mercy Health's Lima (Ohio) market last month. Rieger is set to retire on July 12.
At Adventist Health Sonora in California, Greg McCulloch was promoted to president after serving as the hospital's CFO since 2014.
At Portland-based MaineHealth, Albert Swallow III shared plans to retire as CFO in early 2025.
A few specific inpatient and outpatient services in particular are feeling the effects of lower reimbursements leaving CFOs to strategize.
Lower payer reimbursements have had a big effect on inpatient and outpatient services—but there are ten that are taking the cake.
Recent data from Strata Decision Technology analyzed the cost of care across inpatient and outpatient facilities and narrowed in on rate changes seen between 2021 and 2023. It found that there are certain services that had an operating gap that spanned between an eye-opening -12.1% and -42.9%.
How did we get here?
The report, published by the AHA, explains that underpayments from Medicare and Medicaid totaled nearly $130 billion in 2022, and Medicare paid just 82 cents for every dollar hospitals spent caring for patients. This is resulting in a shortfall of almost $100 billion.
What’s worse news for CFOs though is that those cumulative underpayments in the second half of the last decade increased 40% compared to the first half, and that’s even after adjusting for inflation.
Medicare and Medicaid aren’t the only payer types facing intense reimbursement challenges; payers across the industry have seen a steady decline below costs for reimbursements.
What do the numbers show?
Here are ten services where the reimbursement rates don’t cover the costs of providing care across inpatient and outpatient settings:
Inpatient services
Behavioral health: -34.3% below cost
Nephrology: -34.1%
Burns and wounds: -24.1%
Pulmonology: -19.4%
Infectious disease: -15.3%
Outpatient services
Burns and wounds: -42.9% below cost
Nephrology: -32.3%
Behavioral health: -31.7%
Pulmonology: -17.5%
Infectious disease: -12.1%
What’s the CFO Gameplan?
Rising costs and lower reimbursements are spelling “stress” for CFOs, and while viable solutions can seem elusive, they’re not impossible.
Bill Pack, CFO at Conway Regional Health System and a HealthLeaders CFO Exchange member, recently shared some of his top strategies for battling these prevalent issues in his own health system.
Outside of exploring all cost reduction avenues and negotiating a fair partnership with a payer, Pack points to two other important strategies that he deploys: diversification of services and utilization management and efficiency improvements.
“We are also expanding and adding services that include higher-reimbursed procedures or specialties to offset the lower margins of resource-intensive services,” Pack said.
“We are implementing utilization management processes to ensure that resources are used efficiently,” Pack says. “We are also identifying areas for improvement in care delivery, which lowers costs and improves patient care.”
UnitedHealth is warning investors and other payers of a disturbance to the Medicaid market.
The Medicaid business is under watch, according to UnitedHealth CEO Andrew Witty. At a conference on May 29, Witty told investors that Medicaid managed-care payers are getting hit with low state reimbursements, and it may go on for some time. Shortly after this, UnitedHealth’s stock dipped, also bringing down the Medical-Managed Care group.
"We've come through this prolonged redetermination cycle in Medicaid," Witty said. "Making sure the utilization, and the rate and everything else stay in perfect synchronicity during a multi quarter cycle — there's probably going to be some disturbance around that."
Medicaid Unwinding
In April 2023, states began disenrolling ineligible Medicaid members— ‘Medicaid unwinding’—for the first time since the beginning of the pandemic. The rules preventing states from removing members from their Medicaid plans were peeled back, but surveys found that many were wrongfully disenrolled while payers continued to profit.
One study showed that Medicaid fee-for-service physician payments are about 30% lower than Medicare payments, and commercial payments are even lower.
CMS extended Medicaid waivers into 2025, protectingthose who would otherwise be left without coverage. In some states, like Texas and Florida, Medicaid unwinding has left millions without coverage.
A year after Medicaid unwinding began, 22.4 million people have been disenrolled from Medicaid through the redetermination process, according to KFF.
UnitedHealth
Medicaid reimbursements are coming as states continue to determine member eligibility,; drastically cutting beneficiary rolls over the past year.
Witty’s comments indicate the state reimbursements will need to reflect Medicaid per-patient costs, but this could take some time to figure out. Speaking to investors at the conference, Witty also said that this may mean a “multi-quarter cycle” for states to begin paying Medicaid premium rates that are adequate enough to meet the cost of coverage for Medicaid patients, Bloomberg reported.
Utilization is the top concern, as it's currently the primary driver of medical costs. This uptick in costs has accelerated spending on benefits and also hurt Medicare Advantage plan profits. Just this week, UnitedHealth’s stock dropped about 4%, leaving it at $484.72, making it the worst performing stock in the Dow Jones Industrial Average.
The stock of other insurers, like Molina Healthcare and Cetene, also fell this week. UnitedHealth’s stock dropped to a six-week low, despite the insurer’s favorable first quarter earnings, which pacified investor apprehension toward Medicare Advantage and unease after the Change Healthcare cyberattack.
A couple of industry shifts have driven the rapid expanse of health technology.
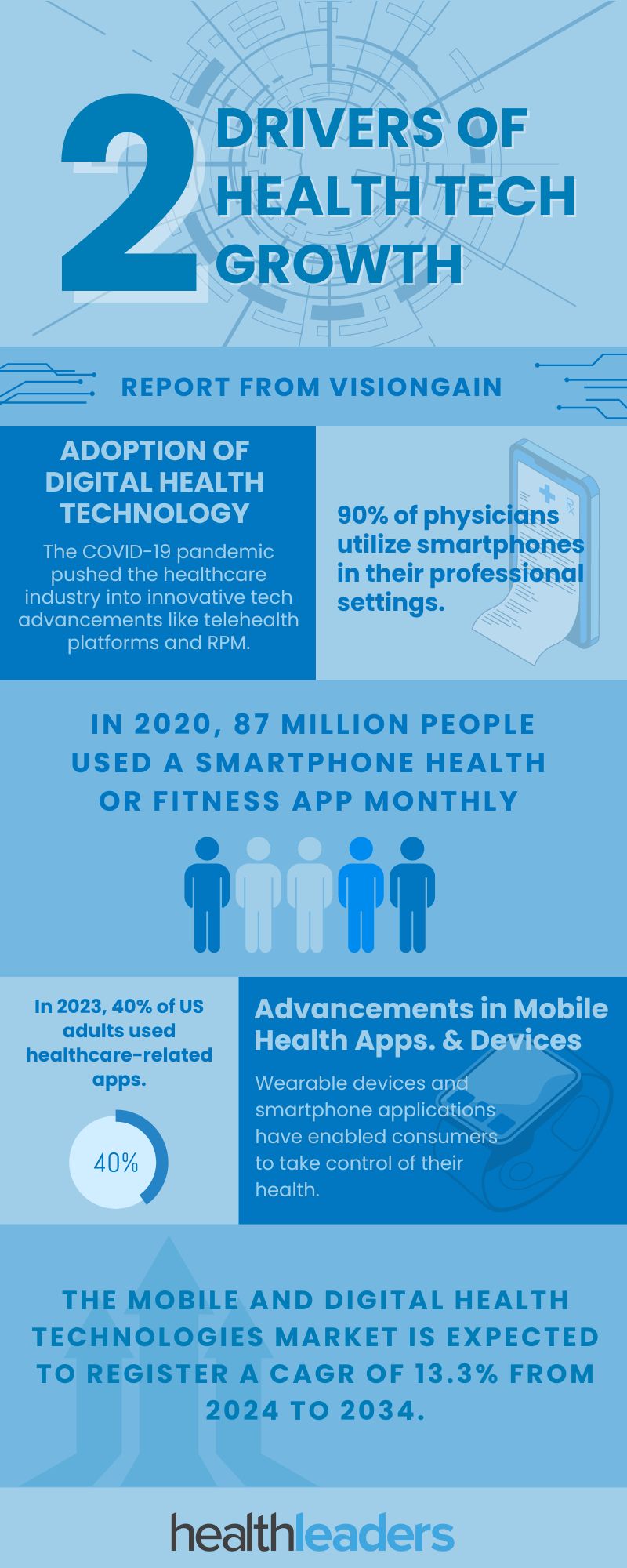
A new report published by Visiongain titled the Mobile and Digital Health Technologies Market Report 2024-2034 has detailed the expansion of health tech. The report cites that the mobile and digital health technologies market is estimated at US$250.8 billion in 2024 and is expected to register a CAGR of 13.3% from 2024 to 2034.
There are two main items behind this market growth: adoption of digital health technology and advancements in mobile health applications and devices.
Adoption of Digital Health Technology
The healthcare industry has made big leaps in the last couple of years in adapting digital health technologies. The advancements the industry has seen are in part due to the adaptations taken around the COVID-19 pandemic. The pandemic pushed the industry to rapidly expand the use of remote care, making telemedicine platforms and remote patient monitoring the norm. Both of these items have equipped providers with much more accessible to their patients in a convenient method.
Advancements in Mobile Health Apps. & Devices
The report cites advancements in mobile health applications and devices as one of the main drivers of growth and innovation in the healthcare market. These new innovations have harnessed the convenience and widespread availability and functionalities of smartphones, and wearable devices to transform healthcare delivery and enable consumers to take control over their health and wellness. From symptom tracking to medication management, wearable devices and health applications have helped bring healthcare into a modern era where consumers can make use of the tech that already surrounds them.
A report from The International Telecommunication Union (ITU) cites that 90% of physicians utilize smartphones in their professional settings, and the majority of individuals rely on their devices like smartphones to access health-related information.
According to a Morning Consult survey in 2023, 40% of US adults used healthcare-related apps, which is a 6% increase from 2018.
Many health systems and patients have struggled with prior authorization procedures.
Prior authorization practices are staying in the spotlight. Health systems are looking for payers to do more to enhance the prior authorization process. While some health insurers have made strides, several states and health systems took matters into their own hands. From partnerships to policy reform, check out our five updates on prior authorization for payers.
In April Humana expanded its partnership with Cohere Health’s prior authorization platform for diagnostic imaging and sleep services. We reported on this partnership last month, read the full coverage.
A Kodiak Solutions report details that the final denial rate for inpatient claims in 2023 was more than 50 percent above the same rate in 2021.
Vermont governor Phil Scott signs a prior authorization reform bill. Among the items in the legislation, it requires health insurers to decide prior authorizations within 24 hours for urgent situations and two business days for nonurgent care.
At the start of this year Oregon-based St. Charles Health System partnered with insurer PacificSource to launch a pilot program to streamline automatic coverage approval for patients in need of cancer treatment.
Oklahoma signed a bill into law that changes several prior authorization procedures including approval timelines. It also requires payers to have prior authorization procedures published on the company’s websites to be available for patients and providers
A not-so-new feud between NewYork-Presbyterian Hospital and union health fund 32BJ has reached a fever pitch. The union fund was on the cusp of signing with Aetna to cover its 210,000 members when a hospital-sized roadblock popped up.
Due to the hospital's prices, 32BJ wanted to exclude it in its new contract. However, Aetna’s contract requires the insurer to get a signoff from the hospital in order to omit it from a client's plan.
According to New York Presbyterian, 32BJ owes the health system over $25 million in medical service bills and is barring 32BJ from signing with Aetna until those bills are covered. Without the payment, Aetna can’t offer the plan the union fund wants.
32BJ says it has no current plans to pay the hospital.
“We were totally shocked. That’s just not how business is done,” said Peter Goldberger, executive director of the union’s benefit funds, speaking to the Wall Street Journal. He added that NewYork-Presbyterian never brought up the charges prior to the union fund attempting to sign with Aetna.
The union health plan spends about $1.5 billion a year covering members—who typically hold occupations such as cleaners, maintenance workers and airport staffers—and their families.
Last year the union health fund spent roughly $22.5 million on care at NewYork-Presbyterian alone.
This led 32BJ to call off signing with Aetna, who they said they do not blame for the situation.
The union fund will continue with its current partner Elevance’s Anthem, which has not included NewYork-Presbyterian in its network since 2022.
The Price Problem
NewYork-Presbyterian’s prices reflect those of big hospitals that command premium rates with private insurers. These demands are high, and sometimes guarantee that the health system will be included in all of an insurer’s networks, even if a client doesn’t want them.
Contract terms like these negatively affect insurer’s clients, usually employers and unions, making it harder for them to guide patients to lower-priced health systems. Employers end up staying in them, despite not knowing what they are paying, and services potentially costing double what the government would pay.
Hospital prices have been a major pain point lately, and data shows they usually pay far more than Medicare rates. There’s also been pushback from other groups that say Medicare rates are far too low and don’t cover the cost of care. Regardless of where the numbers fall, employers need access to pricing data for their health plans.
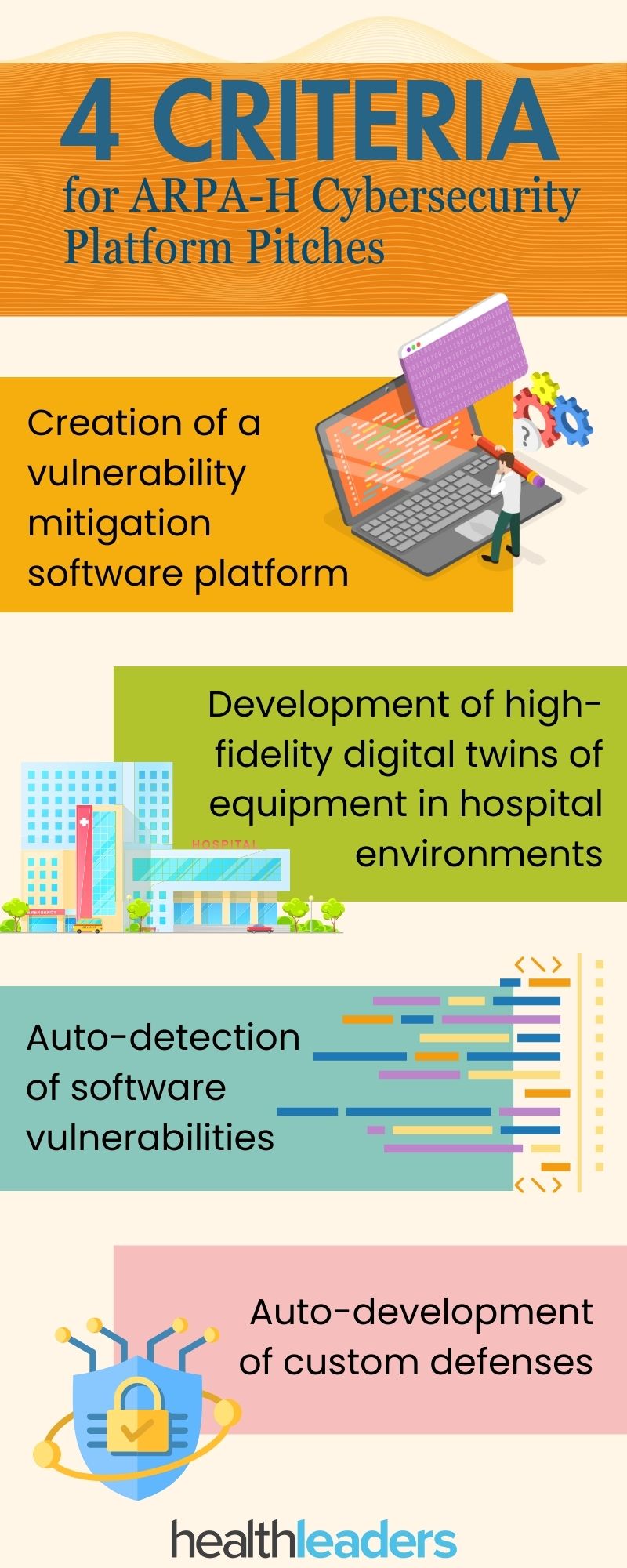
On Monday the HHS research funding agency Advanced Research Projects Agency for Health (ARPA-H) unveiled its Universal PatchinG and Remediation for Autonomous DEfense (UPGRADE) program that will offer “multiple awards” to individuals/groups with the best pitches for a scalable cybersecurity platform that can keep the hospitals’ vast digital systems up to date.
The program hopes to implement a platform that will enhance and automate cybersecurity for healthcare facilities.
“It’s particularly challenging to model all the complexities of the software systems used in a given healthcare facility, and this limitation can leave hospitals and clinics uniquely open to ransomware attacks,” UPGRADE Program Manager Andrew Carney said in a release. “With UPGRADE, we want to reduce the effort it takes to secure hospital equipment and guarantee that devices are safe and functional so that healthcare providers can focus on patient care.”
The U.S. healthcare system struggles with continuously updating the security technology that is put in place. The release noted that when updating critical hospital systems, taking that system offline can be “very disruptive.” This often leaves vital data open for hackers and ransomware groups.
The UPGRADE program aims to address these issues by choosing a new platform that can proactively probe for vulnerabilities. While the agency is holding a Virtual Proposers Day on June 20, it has not yet announced open and closed dates for this solicitation.
There are four technical areas that the ARPA-H will be seeking in these outside proposals. This infographic breaks it down.










9b3a.jpg?itok=Bno3PUQ6)