U.S. health system spending on social determinants of health could jump even higher.
Health systems are struggling to find a strategy to identify and address social determinants of health.
A study by Deloitte shows that in the U.S. health inequities cost the healthcare industry roughly $320 billion every year. By 2040 that could jump to $1 trillion if the industry fails to take action.
To address this, health systems would have to understand why they spend thousands of dollars more each year to treat minorities for the same chronic conditions seen in white patients.
Check out the accompanying article and a new AI based tool that may be able to help here.
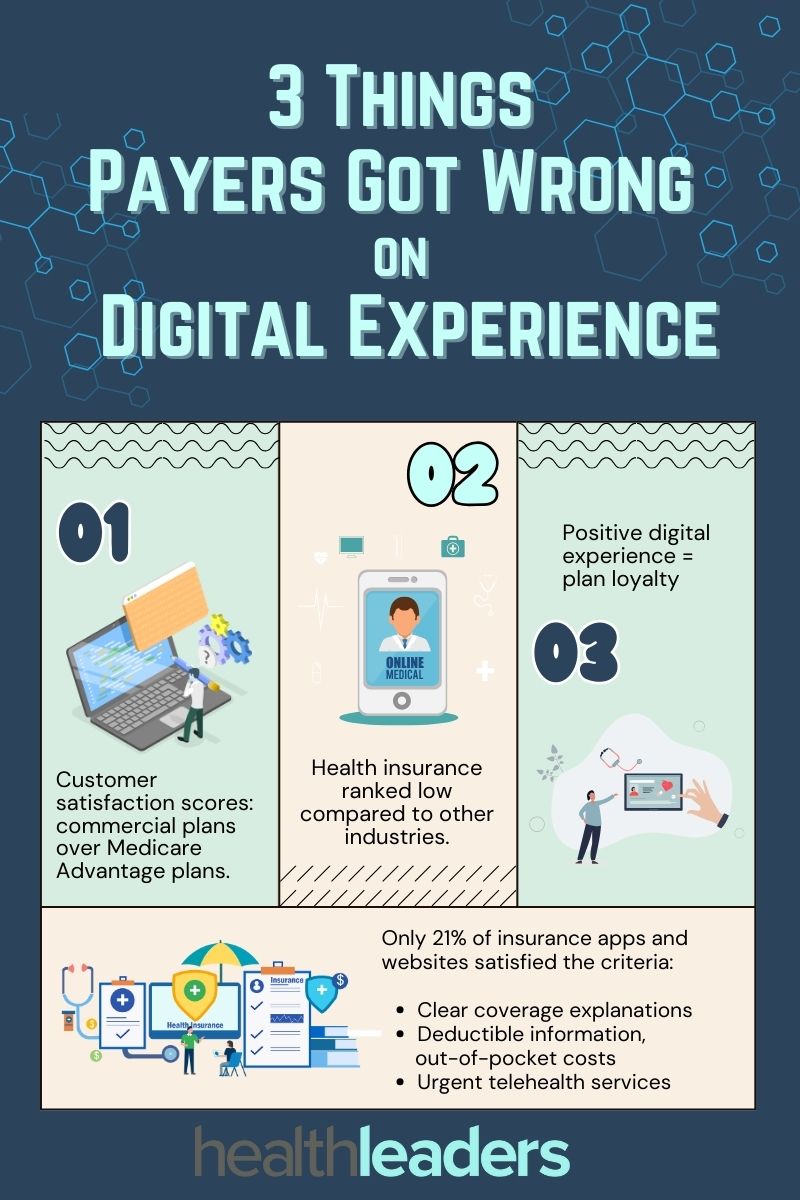
Digital experiences in healthcare have progressed exponentially over the last few years: from administrative AI to smartphone app diagnosis, but payers seem to have fallen behind in this realm. According to a J.D. Power report, the digital insurance experience isn’t where it should be.
J.D. Power defines four basic functions of apps and websites, including: digital functionality, organization and visual appeal. Out of the 5,590 members that were surveyed, including the 14 largest Medicare Advantage plans and 15 of the largest commercial member health plans, roughly one third of insurer’s apps and websites failed on these basic functions.
Overall only 21% of the digital properties met all the criteria to be considered high-functioning digital solutions, such as clear explanations of coverage, provided information on deductibles and out-of-pocket costs, and offering urgent telehealth services.
Here are three notes on the digital insurance experience:
Commercial plan members had a better digital experience than MA plan members, and overall rated it more highly: commercial plan apps and websites had an average customer satisfaction rating 646 out of 1,000, compared to 629 for MA plans.
Health insurers ranked low for digital experience compared to other industry scores. Property and casualty insurance averaged a score of 700 for customer satisfaction, and self-directed wealth management apps had a score of 718.
When MA plan members had a positive digital experience, it was linked with their intent to stay with the plan. In MA plans that received scores of 801 or higher, 89% of members said they would definitely stick with the same plan.
Medicaid unwinding left millions uninsured, particularly children, Black, Hispanic and lower income communities.
Roughly one quarter of Americans who were disenrolled from their pre-pandemic Medicaid coverage are now completely uninsured. Why? High costs and other procedural hurdles that particularly affect minorities and lower income communities who rely heavily on federally funded coverage. Plainly, health coverage is too expensive and trying to prove eligibility can sometimes feel like a fool’s errand.
The provision that kept states from disenrolling consumers from Medicaid during the COVID-19 pandemic ended in March 2023. The Biden administration projected about 15 million people would lose their coverage, but 20 million did instead, according to a Kaiser Family Foundation report. Most states will have until June to continue conducting eligibility reviews, and that 20 million is expected to grow.
The Fight for Coverage
The biggest hurdle for acquiring coverage for more than half (54%) of uninsured adults is simply cost. KFF’s survey looked at over 1,200 adults in February and March 2024, including individuals who stated they had Medicaid coverage in early 2023, prior to the ending of pandemic eligibility rules in April 2023.
Two-thirds (64%) of individuals who were enrolled in Medicaid before the unwinding process began say they took action in 2023 to renew their coverage. The survey found that about one-fifth of all individuals who had Medicaid coverage in early 2023 were disenrolled sometime later that year. Over one-third who attempted to regain any type of coverage said the process was difficult, and about half (48%) called it stressful.
Long call center wait times, excessive paperwork and uncertainty about what paperwork was needed were common complaints. Some states that have not expanded Medicaid require proof of residency in order to renew coverage, creating yet another hurdle. The survey shows that individuals living in non-expansion states were at least twenty percentage points more likely to say they were asked to submit proof of residency. If the state is unable to obtain eligibility documents electronically, then they may put the task back on the enrollee to submit these documents.
Additionally, Black and Hispanic groups were much more likely than White groups to say they were asked to submit proof of residency to regain coverage: Black groups (71%), Hispanic groups (60%), and White groups (42%).
A recent KFF tracking poll also found that seven out of ten of the overall public (69%) said they heard only “a little” or “nothing at all” surrounding state removals of enrollees from Medicaid as pandemic provisions came to an end.
The survey showed that groups with lower levels of education, particularly those with a high school diploma or less, were far more likely to say they heard “nothing at all” about states removing enrollees from Medicaid.
Apart from administration processing issues and procedural hurdles on Medicaid’s end, among those who took action to renew their coverage, about 14% said they did not have reliable internet access to complete the forms online.
The survey also shows the clear and immediate impact of loss of coverage on health: over half (56%) of individuals surveyed said they missed a necessary healthcare appointment or skipped their prescriptions as they waited to regain coverage.
Who’s Most Affected?
Medicaid enrollment jumped by almost one-third during the pandemic, from 71 million in February 2020 to 94 million in April 2023. But this data isn’t complete, as it doesn’t reflect one of the largest groups affected by Medicaid coverage loss: children.
Children have the highest official poverty rates of any age group. In 2022 about 16% of children aged 0-18 were living in poverty, according to a KFF news report. Furthermore, the report states that in 2022 supplemental poverty rates were the highest for asian children (25.9%), hispanic children (19.5%), and black children (17.8%).
KFF news released a report on April 15 that showed in Texas two million consumers were disenrolled from Medicaid in March 2024, and 1.34 million of those individuals were, you guessed it, children.
The Fix
Overall, those still on Medicaid rate the program positively across all groups. The survey shows that ratings are also consistently positive in both expansion and non-expansion states. Individuals are happy with Medicaid coverage, all things considered. The issue is in acquisition.
As of now, roughly 30 million individuals are still awaiting Medicaid renewals.
Is there room for payers to intervene here? With millions losing coverage, is there any opportunity for payers to put forth new plans or aid in offering affordable supplemental coverage that targets these groups? Maybe, but not without federal allyship, and not without reexamination of this important federally funded coverage, and the procedural barriers that accommodate it.
Payers and providers shouldn't underestimate the value of streamlined, accurate data, especially when it comes to contract negotiations.
HealthLeaders sat down with Britt Barrett, managing director and teaching professor at Brigham Young University and former CEO with HCA, Texas Health Resources, and SHARP, to discuss what needs to be done in order for data to be leveraged for both payers and providers in contract negotiations.
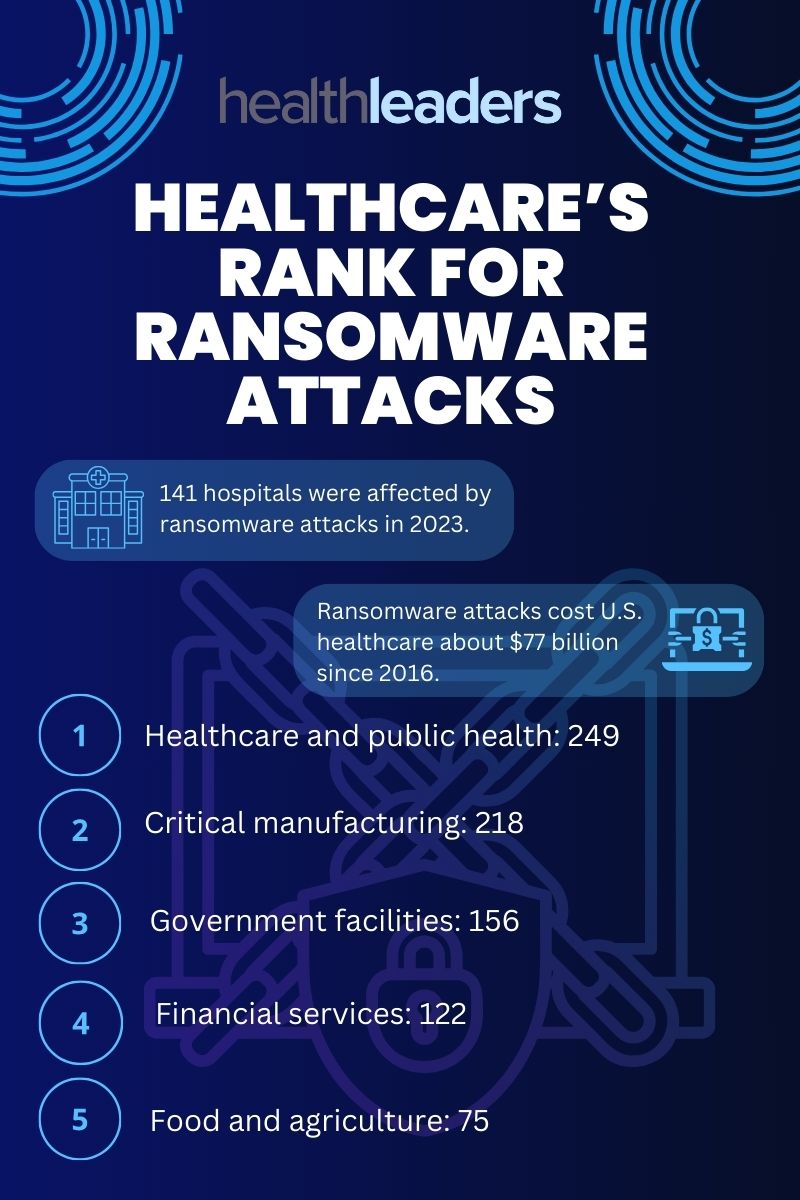
Healthcare has a big target on its back when it comes to ransomware attacks.
Ransomware attacks affect dozens of different sectors, but healthcare seems to be a particular favorite. An analysis published by EmsiSoft looked at just how big the ransomware problem is for hospitals and health systems.
Firstly, ransomware attacks are difficult to gather data on because many of them aren’t recognized as ransomware attacks. “Encryption events” is a term often used which can make tracking these events a challenge, reported cybersecurity firm Emsisoft.
In 2023 over 2,000 hospitals, schools and governments were directly impacted by ransomware attacks. The Change Healthcare attack is just the latest in the mix, and now they may even be facing another one.
At least 141 hospitals were affected by ransomware attacks last year, and cost U.S. healthcare organizations about $77 billion in downtime alone since 2016.
So far, despite government task forces, asset seizures and arrests have been implemented, but ransomware attacks persist. One solution may even be to outright ban the payment of ransoms, according to Emsisoft, stating in a blog post: “If it is made unprofitable, most attacks will quickly stop.”
The massive issue is only set to worsen unless health tech experts can find viable solutions to protect health systems from these attacks. Check out this infographic for a breakdown of where healthcare falls in ransomware attacks.
Medicare Advantage has gone through numerous changes and hurdles since its creation.
The recent rate cut to Medicare Advantage is the biggest change we’ve seen to the program since 1997. Created over thirty years ago, Medicare Advantage has gone through much evolution, ups and downs of popularity, and regulation pressures since it began. With the original intention of giving consumers a Medicare option beyond the traditional fee-for-service program, and bringing the financial savings and efficiencies in managed care in the private sector, MA has become a public favorite in recent years with higher utilization.
MA has generally been more expensive than Traditional Medicare, and those overpayments have increased in recent years. In 2019 MA spending was up an estimated $7 billion compared to Traditional Medicare.
The recent rate cut to MA signals a significant shift in the program that has been a public favorite in recent years. For the payer, this change could impact business by potentially reducing overpayments and increasing competition within the MA market.
It is important for payer c-suite leaders to closely monitor these developments and adjust strategies accordingly to remain competitive in the evolving landscape.
Take a look at how MA has changed over time since its creation.
Medicare Advantage Timeline
1982: Tax Equity and Fiscal Responsibility Act (TEFRA) authorizes Medicare to contract with risk-based private health plans.
1985: Rules to implement risk-based contracting are completed and Medicare Part C begins.
1997: Balanced Budget Act: program renamed to Medicare + Choice: Medicare payments are reformed by extending per-case payment methods to all categories of post-acute care.
2000: Benefits Improvement and Protection Act (BIPA) restores approximately $11.5 billion over five years to hospitals under Medicare, Medicaid, and other federal and state health care programs, but fails to reverse the declining participation of Medicare plans and the enrollment of beneficiaries.
2003: Medicare Modernization Act: Name changed to Medicare Advantage.
2010: Reductions in MA payments are made by Patient Protection and Affordable Care Act.
The new rate cut will have a strong impact, but not on big payers.
Just about every insurer is up in arms over the new Medicare Advantage rate cuts.
To recap: MA plans will see a base rate cut of 0.16% in 2025 since risk scores are expected to be 3.86%. The expected average change in revenue will be 3.7%, and CMS notes that “this is an increase of over $16 billion in 2025 compared to 2024 in expected MA payments.”
However, this rate cut isn’t going to be a huge blow to big payers. Yes, we saw their stocks take a dive when it was announced, but it won’t be detrimental to their business.
MA insurers started the 2023 year financially stable, even considering the uptick in utilization late in the year. The giants still showed strong profits in the billions: Humana at $2.5 billion, Cigna at $5.2 billion, UnitedHealth at $22.4 billion, Elevance at $6 billion, Centene at $2.7 billion, CVS (Aetna) at $8.3 billion…you get the picture.
The rate cut is still a big deal. It's the biggest change in Medicare since Medicare Choice was included in the Balanced Budget Act of 1997, which reformed Medicare payments by extending per-case payment methods to all categories of post-acute care.
Pressure for small insurers
It will be a bigger deal for smaller insurers. Industry expert Paul Keckley dives into who will be most affected by this MA change in his Keckley Report. A few groups he says will feel the brunt of the change are:
Smaller Medicare Advantage sponsors and their lobbying groups will take a hit after trying their best to defeat this rule and members will pay dues for the results.
Hospitals and physicians will feel the effect of this rule in the form of reimbursement cuts to care providers, especially smaller and rural health systems with large MA enrollment.
MA brokers, agents and marketing companies may feel a hit to their profits from constraints of MA marketing tactics and member transparency protections. These could reduce revenue for third-party marketing organizations that sell their services to these plans. Keckley says that a shakeout is likely.
MA enrollees may see fewer plan options and higher premiums, thickening the barrier to access affordable healthcare. Although the ruling adds benefits for behavioral health and data privacy protections, it most likely won’t outweigh the stiffening premiums and fewer plan options. Keckley says that while big MA plans will be hurt but will adapt, while small plans will be left in the dust.
Supplemental service providers will see lower payments from CMS and may be forced to reduce or eliminate supplemental benefits that aren’t as important to members. Keckley surmises that benefits like fitness programs may be cut, but dental and prescription drug benefits appear to be safe.
Lastly, the 2024 Presidential campaign is happening right alongside this MA change and Keckley says that he has no doubt the campaigns “will opine to Medicare security in their closing rhetoric recognizing MA covers more than half its enrollees.” MA insurers will submit their new plans to CMS by June 3 and open enrollment begins in October, a month before the nation votes for the next president.
Overall, this MA rule will affect all plans in one way or another, whether it’s day to day operations, heightening friction with providers or reimbursement negotiations, Keckley concludes in his report that MA is simply a work in progress.
CMS announced it will continue with its 0.16% rate cut for Medicare Advantage plans insurers.
The Medicare Advantage rate cut proposed in January is here to stay, and payers are not happy.
CMS announced the finalization of the 0.16% rate decrease on Monday, to the disappointment of payers and their investors.
Insurer stocks immediately began to drop, with Humana seeing a nearly 10% drop, CVS Health dropping 5.9%, UnitedHealth decreasing by 4.5%, and Elevance dropping 4%. The stock performance plays into the growing concern amongst investors that Medicare Advantage will continuously face more regulatory and earnings pressure in the future.
With the new rate, next year Medicare Advantage payment cuts could drop by 1% per month per beneficiary, according to a study from the payer lobbying group Better Medicine Alliance, which represents payers in Medicare.
What does it all mean?
Medicare Advantage has seen an unusual rise in medical costs recently, with higher utilization to blame, and insurers are arguing the CMS did not factor in these rising costs that plans are facing when it calculated the new rate. Some payers are arguing that the new rate will hurt seniors, who have been responsible for the higher utilization rates that Medicare Advantage has been seeing.
Medicare Advantage has been a hot topic as of late, with several factors shaking up the market and feelings of uncertainty about how the market will perform in 2024 and 2025. The Biden Administration’s crackdown on upcoding practices is one factor that slowed the original excitement and popularity around Medicare Advantage.
Just last week HealthLeaders reported on the strength of the Medicare Advantage market, with a Chartis study revealing strong potential and stability as enrollment grows. The growth comes on the heels of a big Medicare Advantage milestone: over 50% of Medicare-eligible persons enrolling in a Medicare Advantage plan. With these factors, the optimism of insurance executives prevails.
Other influential factors include an aging population that will most likely continue the high utilization rates. Procedures like knee and hip replacements for seniors are two of the main operation utilizations that are seeing an uptick. Tougher star ratings have also played into the Medicare Advantage payer landscape, with many seeing a decrease in their ratings. Broker constraints and opportunities in special needs plans may also have some effect on payers in the MA space.
Payers may be in a rush to exit the Medicare Advantage market as they see its profitability declining, but this may not take place immediately. Medicare Advantage is still a massive part of the health insurance market that stands to continue profitability if payers can pivot their strategies, get creative with existing opportunities, and play with a straightforward hand.
The 2024-2030 plan lays out strategic goals and principles to help the health IT sector.
Last week the ONC released a strategic plan that outlines health IT priorities with a focus on health equity and AI use over the next five years. The plan intends to serve as a guide for federal health IT initiatives, as well as an impetus for activity in the private sector.
According to the ONC and HHS, the plan, which is a collaboration of the ONC with 25 other federal agencies, outlines federal health IT goals to improve health experiences and outcomes for individuals and populations as a whole.
The plan cites that its intended use aims to: prioritize resources, align and coordinate efforts, benchmark and assess progress, and signal priorities to the industry.
The plan outlines four main goals:
1. Health and wellness: Promote health and wellness for individuals, communities and populations so they feel empowered to manage their health.
2. Enhance the delivery and experience of care: Enhance the delivery of care for everyone from patients to providers to public health experts.
3. Accelerate research and innovation: Accelerate research and innovation through collaborative efforts across health IT developers and users.
4. Connect the health system with health data: Connect the health system with health data for all health IT users
Goals 1-3 are focused on plans to improve the experiences and outcomes for health IT users, while goal four focused on the policies and technologies needed to support those users.
The plan also outlines six principles including:
Person-centered, inclusive design to “strengthen individuals’ ability to securely access and use their own health information to take greater control over their own health, while ensuring that their data are accurate.”
Safety and quality to “promote the use of health data that are accurate and provide benefits to individuals and their communities.”
Privacy and security to “provide tools, guidance, and regulations to build trust and protect individuals’ health information from misuse.”
Data-led decision making to support health information sharing throughout the healthcare industry in order for groups, organizations and individuals make informed decisions and create better health outcomes.
Increase health equity across all populations to “advance the use of data to represent social needs and the conditions in which people live, learn, work, and play.”
Encourage innovation and competition to support “new solutions and business models for better care and improved outcomes.”
"The draft plan acknowledges the swift evolution of AI and increased use in health care, emphasizing the urgent need for the federal government to navigate this transformative landscape both responsibly and effectively in health and health care," ONC officials wrote in a blog post.
The affordability of health coverage is often a barrier for many.
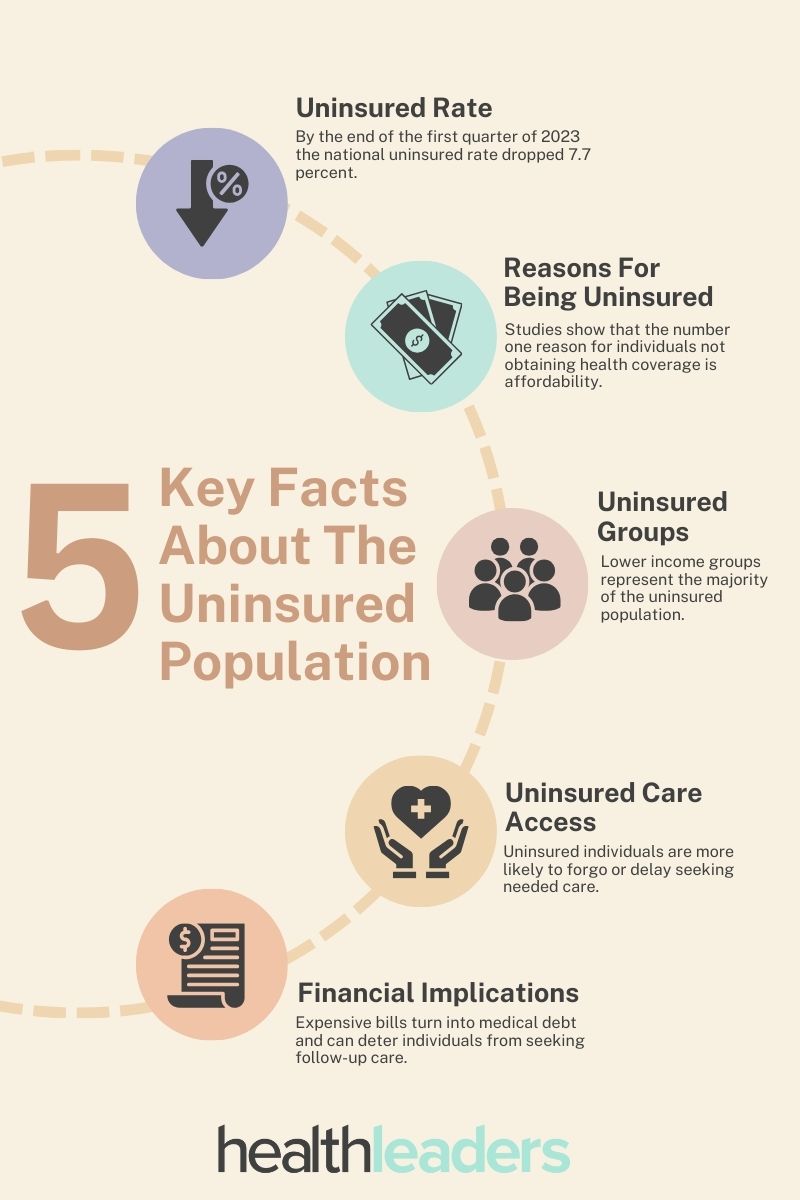
The number of uninsured individuals in the US has slowly dropped over the last few years. Initiatives like the Affordable Care Act and enhanced subsidies in the Marketplace have helped millions obtain affordable coverage.
By the end of the first quarter of 2023 the national uninsured rate dropped 7.7 percent. Between 2020 and 2023 the total number of uninsured Americans declined from 31.6 million to 25.3 million.
The group with the highest enrollment rate were individuals whose income was either below 100 percent or between 200 and 400 percent of the federal poverty level. Racial and ethnic disparities in health coverage also persist, despite enrollment gains over time.
According to KFF, the cost of insurance is the number one reason for individuals not purchasing coverage is affordability. In 2022, 64 percent of nonelderly uninsured adults cited the high cost of coverage as their main reason for not purchasing insurance.
Many also cannot access coverage through their jobs, in states that did not expand Medicaid, many lower-income adults still remain ineligible for financial assistance for coverage. Up until recently, undocumented immigrants were eligible for federally funded health insurance, but some states like California, Oregon and Washington have taken aim at this issue and have offered extended coverage to immigrants.
The Biden administration has made healthcare a major focus of its term, and that has certainly played a role in increased enrollment. The significant enrollment gains in 2021-2023 can be associated with the administration’s policies to support health insurance expansion.
Individuals who do not have health coverage often forgo or delay seeking needed care and this only exacerbates the healthcare needs of the nation, leading to more hospitalizations and care team burnout. Numerous studies repeatedly show that uninsured individuals are less likely than the insured to seek or receive preventative care and other services for major health concerns and chronic diseases like diabetes and heart conditions.
Not being able to secure health coverage can have massive financial implications. When individuals without insurance do seek care, they're often faced with expensive bills that they cannot afford. Since most of the insured population is a lower-income group, seeking care can quickly turn into medical debt affecting other financial aspects of the individual's life and possibly deter them from seeking follow-up care.



77df.jpg?itok=A9hPSH8c)
46fc.jpg?itok=Cld0-cnH)

9d79.jpg?itok=OaI2oj43)
2679.jpg?itok=stlUP70Q)
c3da.jpg?itok=SjGesKZU)


e40c.jpg?itok=FenmC-E5)